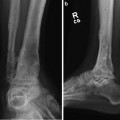
Fig. 1
Post-traumatic ankle arthritis. LDTA 98°. Talocrural angle 73°. No fibular deformity in the frontal plane. Contralateral ankle: LDTA 89° and talocrural angle 78°

Fig. 2
Distal tibial deformity with ADTA 60° and 17° fibula apex posterior angulation (contralateral side 8° for total of 9° apex posterior deformity)
Fig. 3
(a, b) Pre-operative deformity diagram. Tibial mechanical axes showing the proximal mechanical axis (blue line) and the distal mechanical axis (red line). Origin (O) is placed at the CORA. Corresponding point (C) is the intersection of “T” perpendicular to PMA
3 Preoperative Problem List
1.
Distal tibia malunion
2.
Partial fibula malunion
3.
Post-traumatic ankle arthritis
4.
Fixed equinus compensation
4 Treatment Strategy
This patient was relatively young, ankle ROM was preserved, and he maintained high activity level. Therefore, a joint-preserving treatment strategy was employed with deformity correction and ankle distraction arthroplasty. Surgical treatment included an open anterior distal tibial exostectomy and a percutaneous distal tibial osteotomy (Gigli saw technique). Gradual tibial correction was accomplished with a Taylor spatial frame . The foot was incorporated to distract the ankle (performed gradually 1 mm/day for 5 days). Universal Ilizarov hinges were placed on the transmalleolar axis for ankle motion and to address the compensatory equinus deformity (Figs. 4 and 5). A staged fibula osteotomy and frame modification with distal tibia-fibula wire placement were performed once the tibia deformity was equal to fibular deformity (Fig. 6). Continued gradual deformity correction was completed. Throughout deformity correction and osteotomy consolidation, ankle motion and distraction were maintained (Saltzman et al. 2012; Tellisi et al. 2009). Frame removal was performed after bony healing at approximately 14 weeks.

 8: Femoral Bone Defect
8: Femoral Bone Defect
 11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
 22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
 39: Ilizarov Ankle Fusion
39: Ilizarov Ankle Fusion
 84: Lapidus Fusion with External Fixation
84: Lapidus Fusion with External Fixation
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov




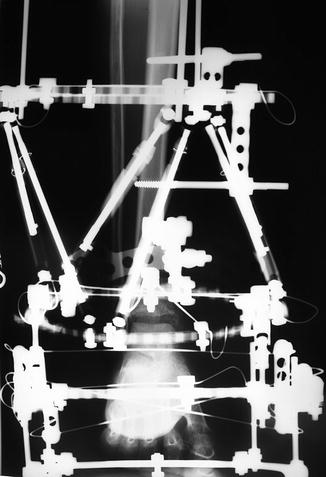
Fig. 4
Intra-operatively, distal reference ring is attached orthogonally. There is no fibula fixation to allow a tibia only deformity correction
Fig. 5
Tibia deformity is partially corrected and equal to fibular deformity. Ankle joint is distracted (5 mm). Hinges are placed at the transmalleolar axis, allowing ankle ROM
Related posts:
8: Femoral Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
39: Ilizarov Ankle Fusion
84: Lapidus Fusion with External Fixation
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
