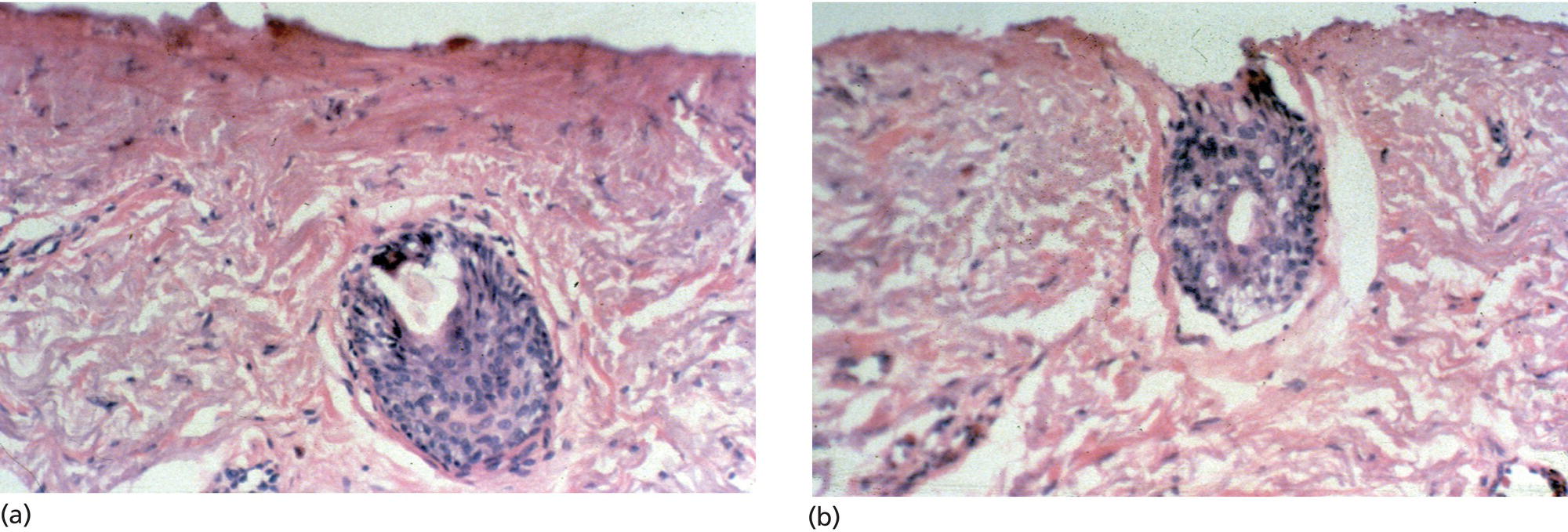
Michael B. Lipp, Kunal Angra, and Mitchel P. Goldman Cosmetic Laser Dermatology, A West Dermatology Company, San Diego, CA, USA Carbon dioxide (CO2) and erbium:yttrium aluminum garnet (Er:YAG) lasers are currently available in two forms: confluent and fractionated. The differences between the results, adverse effects, and downtime are compared and contrasted in this chapter. The modern era of CO2 laser resurfacing began in 1994 with the development of the UltraPulse CO2 laser by Coherent Medical (now Lumenis, Inc., Santa Clara, CA, USA). This laser delivers peak fluence above the ablation threshold of cutaneous tissue (5 J/cm2) with tissue dwell times shorter than the 1 millisecond (ms) thermal relaxation time of the epidermis. These new generation CO2 lasers limited tissue dwell time by either shortening the pulse duration (e.g. UltraPulse) or using scanning technology to rapidly sweep a continuous wave CO2 laser beam over the tissue such that the laser beam does not remain in contact with any particular spot on the tissue for longer than 1 ms (e.g. SilkTouch, Sharplan Laser Corporation, now Lumenis Inc., Santa Clara, CA, USA). These high peak power, short pulsed, and rapidly scanned CO2 laser systems allow laser surgeons to precisely and effectively ablate 20–30 μm of skin per pass while leaving in its wake a considerably smaller residual zone of thermal damage (up to 150 μm) than that left behind by the previous generation of continuous wave CO2 lasers (up to 600 μm). Clinically, this technological advancement translates into superior clinical results and a more favorable safety profile than seen previously with the continuous wave CO2 lasers. The thermal effect of the CO2 laser acts on dermal collagen stimulating neocollagenesis and tightening of facial skin. Successful ablation maximizes thermal stimulation of the dermis while limiting nonspecific thermal damage. Another method used to decrease thermal damage is to follow a session of CO2 laser ablation with the Er:YAG laser. With this technique, the residual nonspecific thermal damage left from the CO2 laser is vaporized by subsequent passes with an Er:YAG laser which leaves little, if any, nonspecific thermal damage. Given the impressive clinical results achieved with the high peak power, short pulsed, and rapidly scanned CO2 lasers, they quickly replaced chemical peels and dermabrasion as the treatment of choice for cutaneous resurfacing. However, the impressive results achieved with these new generation CO2 lasers were not without drawbacks. Reepithelialization can take 5–14 days depending on the depth of ablation [1]. Postoperative transient erythema can last up to 6 weeks and post‐inflammatory hyperpigmentation can last up to 4 months depending on the depth of laser ablation, amount of residual nonspecific thermal damage, and patient’s skin type[2]. Finally, there is a risk of fungal, viral, and bacterial infections on the denuded skin as well as delayed permanent hypopigmentation from destruction of melanocytes and resultant scarring. Minimizing these potential adverse effects requires excellent postoperative care and is time‐consuming for both the patient and physician. These side effects, as well as the significant “downtime” typically associated with CO2 laser resurfacing and extensive postoperative care, are unacceptable to many patients and significantly dampened the initial enthusiasm associated with their use. As the CO2 laser typically operates near its tissue ablation threshold (5 J/cm2), in most resurfacing applications, a large fraction of its energy is invested in heating rather than ablating tissue. Consequently, the CO2 laser produces relatively large residual thermal damage zones and causes significant desiccation of the target tissue after only a few passes. With each subsequent pass, the amount of vaporized tissue decreases while thermal damage increases and a “plateau” of ablation is typically reached after the fourth pass. Nonspecific thermal damage has a negative impact, not only on the CO2 laser’s ablative capacity, but also on its side effect profile. Our research suggests that the relatively large thermally induced residual zone of necrosis (up to 150 μm) left behind by the CO2 laser is one of the main factors contributing to its adverse sequelae including prolonged erythema, postoperative pain, delayed healing, infection, hypopigmentation, and scarring. To minimize the issues resulting from a large residual thermal zone the Er:YAG laser was introduced for resurfacing. While it was successful in reducing thermal damage it was unable to penetrate beyond papillary dermis as a result of its high absorption by water. A multimode Er:YAG system, the tunable resurfacing laser (TRL), was developed (Sciton, Inc., Palo Alto, CA, USA) which allows the user to blend a variety of ablation and thermal coagulation depths by extending the pulse duration of the Er:YAG laser which is typically less than 0.5 ms. Extending the pulse duration to 4–10 ms allowed for less flash vaporization and more prolonged thermal heating to occur. The TRL can be tuned for pure ablation or CO2‐like thermal injury, or any point in between. Modifications of technical protocols have continued to improve clinical outcomes. Combination therapy with CO2 immediately followed by Er:YAG lasers allow cosmetic surgeons to capitalize on the unique benefits of each laser system and to minimize their disadvantages. Er:YAG laser treatment can be used to bypass the ablation “plateau” characteristic of CO2 resurfacing to ablate deeper into the dermis. Improved postoperative healing can also be attained when the short‐pulsed Er:YAG laser is used to remove the residual zone of thermal necrosis left behind after CO2 resurfacing (Figures 51.1 and 51.2). Additionally, the ablative lasers have turned out to be extremely versatile therapeutic tools. Cosmetic surgeons now regularly combine ablative laser resurfacing with other problem‐specific non‐ablative technologies to address multiple cosmetic concerns for the patient in a single treatment session. The efficacy of Q‐switched lasers in the treatment of pigmented lesions is enhanced when these lasers are used before or after ablative resurfacing. Treatment of vascular lesions with the pulsed dye laser, other vascular lasers, or the intense pulsed light has been shown to be extremely successful when performed prior to skin resurfacing with an ablative laser. Despite early reports advising against it, full‐face laser resurfacing is now safely being combined with rhytidectomy, autologous fat transfer and/or the use of dermal filler or biostimulatory agents like Sculptra® Aesthetic (injectable poly‐L‐lactic acid; Galderma Laboratories, L.P. Fort Worth, TX, USA) to achieve a more comprehensive approach to facial rejuvenation. Poly‐L‐lactic acid is usually reconstituted with bacteriostatic sterile water and lidocaine 1%, which can also improve patient comfort due to the lidocaine’s temporary anesthetic effect. To enhance uniform lamellar collagen deposition, we often utilize a variety of neuromodulator agents such as onabotulinumtoxinA (Botox®, Cosmetic; Allergan), AbobotulinumtoxinA (Dysport®, Galderma Laboratories, L.P), incobotulinumtoxinA (Xeomin®, Merz Pharma GmbH & Co. KGaA) or prabotulinumtoxinA‐xvfs (Jeuveau®, Evolus, Inc.) usually a week prior to laser resurfacing to decrease facial muscular movement. Figure 51.1 (a) Two passes of CO2 laser at 7 J/cm2 leaves approximately 70 μm of residual thermal necrosis. (b) Two passes of Er:YAG laser at 10 J/cm2 results in removal of approximately 50 μm of this necrotic tissue. (Source: Carcamo and Goldman (2006) Skin resurfacing with ablative lasers. In: Goldman MP, ed. Cutaneous and Cosmetic Laser Surgery. London: Mosby‐Elsevier. Reproduced with permission.) Pre‐ and posttreatment protocols have also improved. Although some controversy surrounding the topic of antibiotic prophylaxis remains, a number of studies in the last decade have provided relevant information on common pathogens, effective antibiotic, antiviral and antifungal prophylaxis regimens as well as clinical situations at increased risk for infection after cutaneous laser resurfacing [3–7]. Figure 51.2 Combination UltraPulse CO2 (UPCO2) and Er:YAG laser (patient’s right side) showing improvement equal to left side treated with UPCO2 alone. (a) Before treatment; (b) immediately after treatment; (c) 7 days after laser resurfacing; (d) 3 weeks after laser resurfacing; (e) 2 months after resurfacing. (Source: Carcamo and Goldman (2006) Skin resurfacing with ablative lasers. In: Goldman MP, ed. Cutaneous and Cosmetic Laser Surgery. London: Mosby‐Elsevier. Reproduced with permission.) Improved laser wound care regimens have reduced recovery time and decreased morbidity after laser skin resurfacing. The benefits of occlusive dressings in accelerating laser wound healing have been well established [8]. Timely institution of topical medications in the postoperative period is now allowing surgeons to effectively address a number of expected postoperative symptoms and complications including postoperative erythema and edema, pruritus, and post‐inflammatory hyperpigmentation [9]. In a recent review article submitted for publication regarding topical agents post‐laser resurfacing, several topicals have shown benefits with regards to improved healing and cosmesis [10]. These topicals included: thermal spring water (Avene Thermal Spring Water, Pierre Fabre Dermo‐Cosmetique, Paris, France), conjugated linolenic acid (Pomega MDTM, Pomega Inc., San Anselmo, CA, USA), vitamin C/vitamin E/ferulic acid serum (CE Ferulic, SkinCeuticals, Dallas, TX, USA), tripeptide/hexapeptide technology (Regenerating Skin Nectar, Restorative Neck Complex, and Ultra Nourishing Moisturizer with TriHex Technology; ALASTIN Skincare, INC.; Carlsbad, CA, USA), growth factor serum and gel (TNS Essential Serum and Recovery Complex, Skin Medica, Irvine, CA, USA), red deer umbilical cord lining mesenchymal stem cell extract cream and serum (Calecim Multi Action Cream and Serum, Cell Research Corporation, Singapore), silicone‐based gel (Stratacel, Stratapharma AG, Basel, Switzerland), and microparticulate (1‐3, 1‐6 β‐glucan) gel (Glucoprime gel/TR‐987, TR Therapeutics, Reston, VA). These studies were evaluated using the Oxford Center of Evidence Based Medicine guidelines. After review of the level of evidence in these studies the majority of them were found to be below Level 1 evidence, which prevented making any strong recommendations with regard to any particular topical use (Table 51.1). Vitamin C/E ferulic acid serum, red deer umbilical cord lining mesenchymal stem cell extract cream and serum, and microparticulate (1‐3, 1‐6 β‐glucan) gel had the highest levels of evidence (Level 1B). Discussion of the after‐care post‐laser resurfacing is detailed further in the postoperative section. Table 51.1 Level of evidence for post laser resurfacing topicals.
CHAPTER 51
Ablative Laser Resurfacing: Confluent and Fractionated
Introduction
CO2 laser resurfacing

Topical
Clinical studies
Level of evidence
Laser device
Treatment arm
Control arm
Treatment site
Summary
Thermal spring water
Garcia B, Goldman, M, Gold, M. (2007) Comparison of pre and/or postphotodynamic therapy and intense pulsed light treatment protocols for the reduction of postprocedure‐associated symptoms and enhancement of therapeutic efficacy. J Drugs Dermatol: JDD 6, 924‐8
3B
Photodynamic therapy
Avene thermal spring water
Comparative water spray
Face
Patient and investigator pain assessments showed a significant decrease of pain in the ATSW group on day 2 compared to day 0 (p = 0.015; p = 0.021), which was not seen in the comparative water group
Investigator assessment of pruritus demonstrated a significant difference between both groups at days 4 and 7 (p = 0.0385)
Barolet, D, et al. (2009) Beneficial effects of spraying low mineral content thermal spring water after fractional photothermolysis in patients with dermal melasma. J Cosmet Dermatol 8(2), 114–8
2B
Fractional laser
Avene thermal spring water
Face
Patient reports significant reduction in pain, cutaneous dryness, and erythema on the treatment side (p < 0.05)
Investigator assessment noted marked reduction of erythema on the treatment side (p < 0.01)
Sulimovic, L, et al. (2002) Efficacy and safety of a topically applied Avene spring water spray in the healing of facial skin after laser resurfacing. Dermatol Surg 28(5), 415–8
2B
CO2 pulsed laser or erbium Yag laser
Avene thermal spring water, petrolatum ointment
Petrolatum ointment
Face
Patients in the treatment group experienced statistically significant reduction in erythema (p < 0.04), pruritus (p < 0.045), as well as stinging and tightening (p < 0.05)
Conjugated linolenic acid (CLA)
Wu, DC and Goldman, MP (2017) A topical anti‐inflammatory healing regimen utilizing conjugated linolenic acid for use post‐ablative laser resurfacing of the face: a randomized, controlled trial. J Clin Aesthet Dermatol 10(10), 12–7
2B
Fractionated CO2 laser
CLA
1% Dimethicone ointment
Face
Treatment arm had significantly reduced pruritus at post‐procedure days 1 and 3 (p = 0.03 and p = 0.04)
Treatment arm had significantly reduced edema at post‐procedure day 3 (p = 0.04)
CE Ferulic
Waibel J, et al.
1B
Fractional CO2
CE ferrulic
Vehicle control
Face
Less erythema and edema 24–48 hours post‐resurfacing although not statistically significant
Statistically significant higher levels of bFGF expression on CE Ferulic side (p < 0.05) post resurfacing vs control side
Tripeptide/hexapeptide technology
Gold, MH, Sensing, W, and Biron, JA (2019) A topical regimen improves skin healing and aesthetic outcomes when combined with a radiofrequency microneedling procedure. J Cosmet Dermatol.
3B
Microneedling with radiofrequency
Tripeptide/hexapeptide technology
N/A
Neck
Mean baseline investigator photodamage assessment showed statistically significant improvement at days 30 and 90
Investigator global assessments showed significant improvement in skin tone, smoothness, texture, dryness/flakiness, blotchiness, and overall appearance parameters by day 30
Vanaman Wilson, MJ, Bolton, J, and Fabi, SG (2017) A randomized, single‐blinded trial of a tripeptide/hexapeptide healing regimen following laser resurfacing of the face. J Cosmet Dermatol 16(2), 217–22
2B
Fractionated CO2 laser
Tripeptide/hexapeptide technology (alastin procedure enhancement invasive system)
Dimethicone‐based ointment, petrolatum‐based cream, alastin Broad Spectrum SPF 30+ sunscreen, and gentle cleanser
Face
Investigator‐rated healing was better in the treatment group and achieved statistically significant superiority at post‐procedure day 7 (p = 0.01)
Treatment group had less erythema, exudation, tenderness, and burning/stinging at post‐procedure day 3 (p = 0.02, 0.01, 0.02, 0.03, respectively)
Treatment group reported less bruising at post‐procedure day 13 (p = 0.03)
Subject satisfaction was significantly greater in the treatment group at day 84 (p = 0.03)
Robinson, DM and Frulla, AP (2017) Randomized, split‐face/decollete comparative trial of procedure enhancement system for fractional non‐ablative laser resurfacing treatment. J Drugs Dermatol 16(7), 707–10
2B
Fractional non‐ablative thulim‐doped 1927 nm Fraxel dual laser
Tripeptide/hexapeptide technology (alastin procedure enhancement invasive system)
Dimethicone ointment
Face/Décolletage
Blinded investigator assessment showed significant improvement on the treatment side on day 4 onward (p = 0.035)
Blinded investigator assessment showed significant improvement of lentigines and texture on the treatment side at day 4 (p = 0.043 and 0.009)
Patients reports that the treatment side skin “looked better” and “felt better” compared to the control side (p = 0.05)
TNS
Fitzpatrick, RE and Rostan, EF (2003) Reversal of photodamage with topical growth factors: a pilot study J Cosmet Laser Ther 5(1), 25–34
3B
N/A
TNS recovery complex (gel)
N/A
Face
Patients experienced improvement in the periorbital region (p = 0.003)
Patients had objective significantly decreased depth and number of textural irregularities or fine lines
Biopsies demonstrated thickening of epidermis and neocollagenesis of the grenz zone
Mehta, RC, et al. (2008) Reduction in facial photodamage by a topical growth factor product. J Drugs Dermatol 7(9), 864–71
1B
N/A
TNS recovery complex (gel)
Vehicle
Face
At 3 months, treatment group had greater reduction in fine lines and wrinkles than the control group
Recombinant human epidermal growth factor
Techapichetvanich, T, et al. (2018) The effects of recombinant human epidermal growth factor containing ointment on wound healing and post inflammatory hyperpigmentation prevention after fractional ablative skin resurfacing: a split‐face randomized controlled study. J Cosmet Dermatol. 17(5), 756–61
2B
Fractional ablative CO2 laser
rhEGF
Petrolatum ointment
Cheeks
No statistically significant difference in duration of scab shedding, duration of post‐laser erythema, erythema index, and transepidermal water loss
Disphanurat, W, Kaewkes, A and Suthiwartnarueput, W (2019) Comparison between topical recombinant human epidermal growth factor and Aloe vera gel in combination with ablative fractional carbon dioxide laser as treatment for striae alba: a randomized double‐blind trial. Lasers Surg Med.
2B
Fractional ablative CO2 laser
rhEGF
Aloe vera
Striae Alba
No objective statistically significant differences between the two sides
Patients noted greater and statistically significant improvement on the rhEGF side
Red deer umbilical cord lining mesenchymal stem cell extract (RCE)
Alhaddad, M, et al
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access






