5 Cleft Lip Repair: Bilateral
Introduction
The care for a child with bilateral cleft lip and palate (BCLP) is best managed by a collaborative, interdisciplinary cleft team.1 An infant with a BCLP must demonstrate consistent weight gain prior to any presurgical preparations, which might include lip taping, presurgical infant orthopedics, or nasoalveolar molding (NAM) (see Chapter 2). Feeding difficulties and poor weight gain can be signs of associated cardiac, musculoskeletal, or neurologic deformities that should be evaluated by a pediatrician prior to surgery.
The initial repair of the bilateral cleft lip and nasal deformity is just the beginning of years of treatment; however, this step is a very important predictor for the ultimate outcome.2 The repair of the bilateral cleft lip requires particular attention to detail, as millimeters of error during the surgery in infancy are difficult to correct and may burden the child with permanent cleft stigmata. Lip and columellar length, nasal cartilage position, and dental and skeletal deformities are treated sequentially from infancy to adulthood.
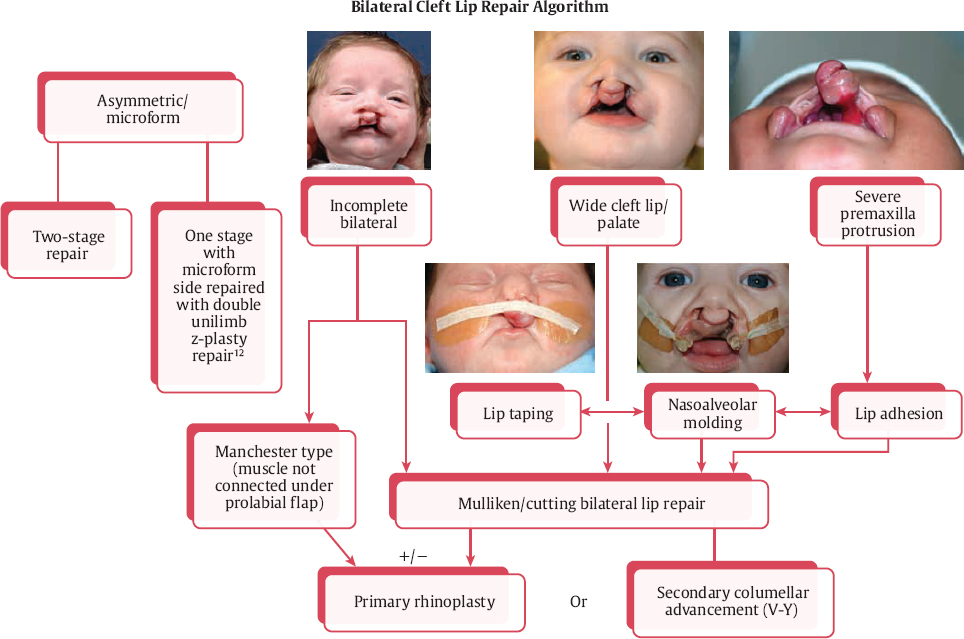
The following core treatment plans and justifications are presented: (1) bilateral lip repair in infancy and a delayed columellar lengthening at later date,3–11 (2) one-stage cleft lip repair +/− primary rhinoplasty (+/− gingivoperiosteoplasty),12–14 or (3) lip adhesion with delayed lip repair in several months.15–18 Presurgical infant orthopedics and/or NAM can be used in conjunction with any of these approaches ( Fig. 5.1 ).
The objectives of this chapter are to orient the reader to the spectrum of types of BCLP and present our preferred treatment algorithms. Supporting evidence is presented for the following: presurgical infant orthopedics unique to the BCLP deformity, techniques and timing for bilateral cleft lip repair and rhinoplasty, and postoperative management protocols.
Historical Perspective
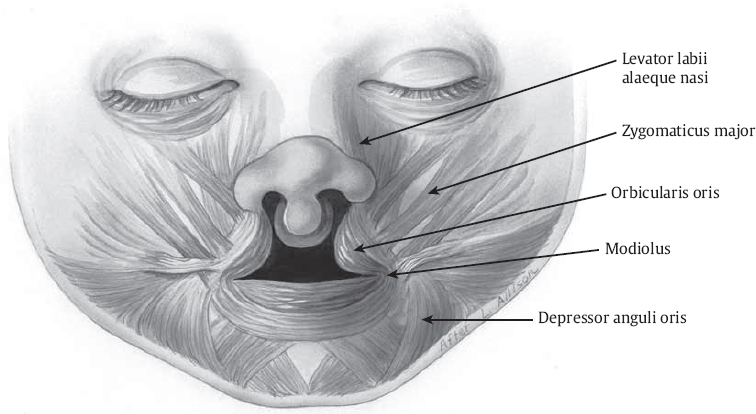
Ridgway and Mulliken pointed out the importance of reconstruction of the philtrum, and the difficulty hereinto. They noted that the “word derives from Greek philtron meaning ‘love potion’… In folklore, the philtrum is believed to represent an indentation left by the finger of God or the spot where an angel put a finger to shush a child.”19 Anatomic studies reveal that the philtrum dimple is probably the result of decussating fibers of the orbicularis oris muscles and the related insertions into the dermis under the philtral columns.20 There is a great variety in the characteristics between individuals, some of which include the philtrum′s shape, size, appearance on actuation, and depth of the dimple. This complexity makes surgical repair of the cleft lip one of the most difficult to master, and one that lifelong learning and evolution for senior surgeons is the norm. The reconstruction of central lip subunit architecture and the growing lip must be considered in the surgical design and application.
Controversy continues as to the effectiveness of presurgical infant orthopedics, NAM, and sequencing of bilateral cleft lip repair. Chen et al. state that “the objective for surgical correction of the bilateral cleft lip is to reconstruct a symmetrically balanced lip and nose with good columellar length.”21 Surgical management of the bilateral cleft lip has evolved over the last few decades. Although nasal and columellar treatment has shifted dramatically, the core principles have been preserved21:
Preserve the presurgical columellar length.
Keep the width of the central lip segment narrow without compromising the blood supply.
Advance the columella prolabium complex superiorly to allow reconstruction of the orbicularis oris muscle behind the prolabium.
Release the alar cartilage attachment from the piriform rim and provide additional coverage of this soft tissue deficiency with the use of inferior turbinate flaps.
Release and reposition the lower lateral cartilage.
Adequately dissect above the maxillary periosteum.
Reconstruct the nasal floor by local mucosal flaps.
Reconstruct the prolabial buccal sulcus with tissue from the prolabium.
Reconstruct the orbicularis muscle sphincter and attach it to the anterior nasal spine.
Reconstruct a new Cupid bow, central vermilion, and lip tubercle with tissue from the lateral lips.
Balance the height of both lateral lips without any incision around the ala and maintain the presurgical nasolabial angle
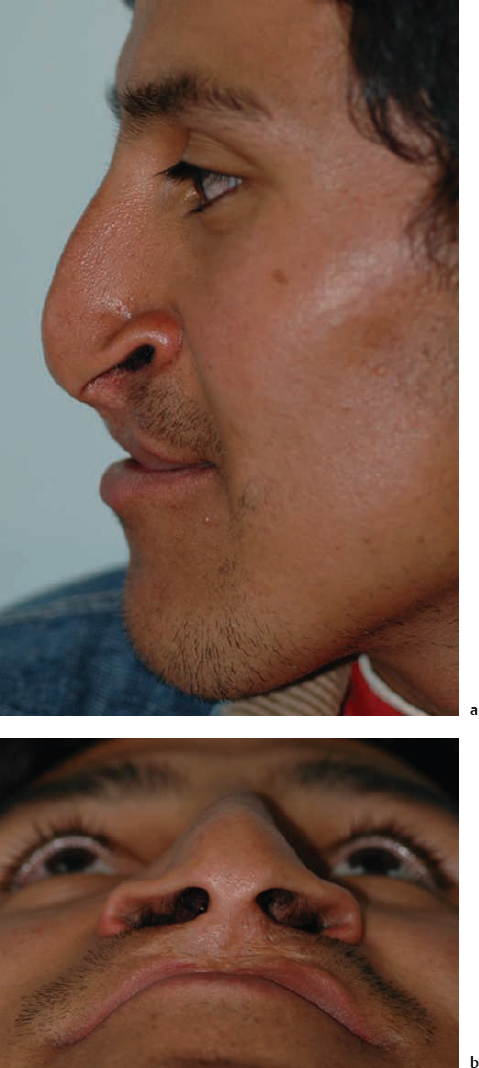
Since the 1950s, the bilateral cleft lip has been repaired in infancy, sometimes with a staged procedure, followed by secondary columella elongation in the first few years of life.3–11 The creation of a natural appearing nasolabial (lip-columellar) relationship has been elusive ( Fig. 5.2 ), resulting in a variety of columellar lengthening procedures that borrow from the lip to lengthen the nose. The laterally based philtral forked flaps can be advanced in a secondary procedure in a V-Y fashion, with or without an active pre-surgical infant orthopedics (e.g., Latham device).7 Mulliken proposed primary rhinoplasty approaches to add columellar length by borrowing from the nostril skin after approximating the splayed lower lateral cartilage domes.22,23 Additional primary rhinoplasty approaches to the nasal tip have demonstrated success, and include open tip rhino-plasty with elevation of the prolabial flap and columella as a unit24 or release of the medial crural cartilages from the caudal septum to access the nasal tip after NAM.14 This presurgical preparation, discussed in Chapter 2, has gained popularity and, along with the primary rhinoplasty techniques, has led to a philosophical and technical shift away from secondary lengthening of the columella, which used skin from the prolabium to add to the columella.
Anatomy
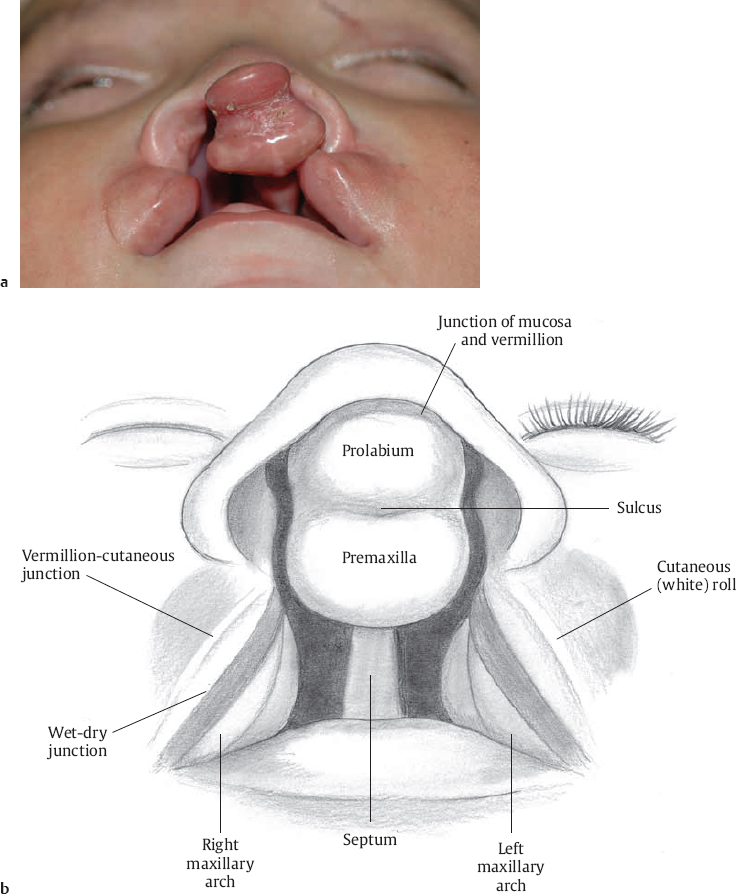
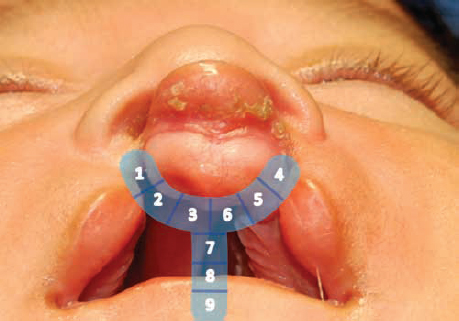
Examination of a neonate with a BCLP should begin with assessment of the symmetry and severity of the lip, premaxilla, prolabium, maxillary alveoli, columella, nasal tip and ala, and palate ( Fig. 5.3 ). Typical patterns of a bilateral cleft lip presentation have fueled various classification schemes. In the Veau classification, a bilateral cleft lip is represented as Group IV or D. In the Kernahan striped-Y classification system, a series of numerical labels are assigned to areas affected by the cleft.25,26 This method allows a consistent numerical method to communicate a cleft type, but is difficult to teach. The bilateral cleft lip, alveolus, and/or palate are represented by the combinations of the numerical values oriented in a Y-shaped configuration with nine subunits ( Fig. 5.4 ):
Areas 1 and 4 represent the nasal floor, right and left, respectively
Areas 2 (right) and 5 (left) represent the lip
Areas 3 (right) and 6 (left) paired alveolar segment
Area 7 the primary palate
Areas 8 and 9 the secondary palate
The authors prefer to state severity (wide/typical/narrow), description (complete/incomplete/microform), and then structure (nasal floor, lip, alveolar cleft, primary and secondary palate). Asymmetry of the lip, nose, or alveolar clefts; presence of a Simonart band; and degree of premaxillary protrusion are noted. One estimate of the severity of the displacement of the premaxilla (and thus the tension on a potential lip repair) is the distance measured between the medial-most edges of the lateral maxillary arches to premaxilla. Mild cases still have contact between the premaxilla and maxillary arches whereas severe cases have ≥ 1 cm of distance ( Fig. 5.5 ).
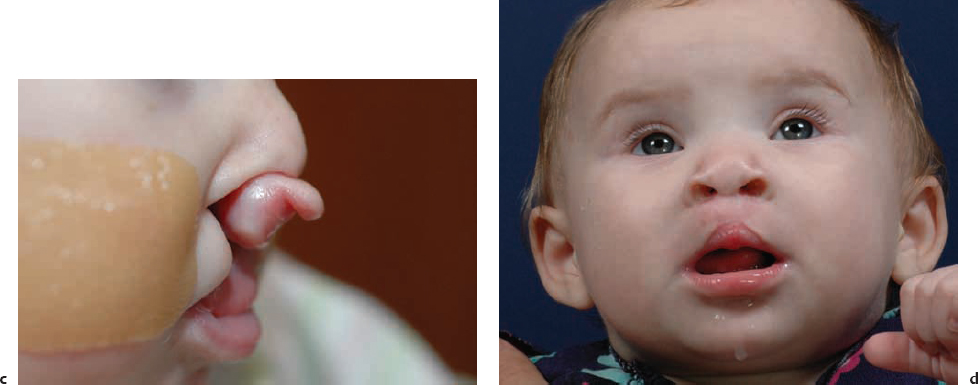
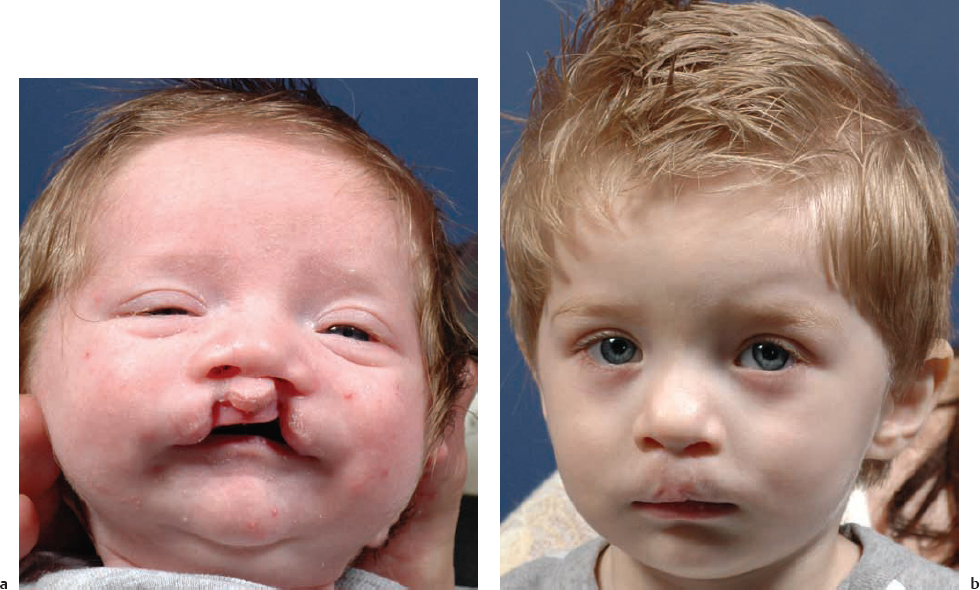
The bilateral cleft lip deformity is usually the most severe and presents with a complete bilateral cleft palate. The varying severities of clefts occur as grossly asymmetric ( Fig. 5.6 ), incomplete, and even microform. Asymmetric bilateral cleft lip deformities can include one or both sides with an incomplete or microform cleft lip ( Fig. 5.7 ), which is the most diminutive form of cleft lip. Rarely, a unilateral cleft palate is seen with bilateral cleft lip. The lateral maxillary segments in a bilateral cleft lip are similar to that in the unilateral deformity, but often with maxillary constriction. The premaxilla in bilateral cleft lip and palate is separated from the lateral maxillary segments and often protrudes anteriorly. The prolabium is the soft tissue formed embryologically by the paired median nasal processes and makes up the central lip. Unlike the unilateral deformity, there is no muscle under the prolabial skin in the complete bilateral cleft lip deformity. In incomplete bilateral cleft lip, the migration of muscle into the central prolabium often occurs. The nasal columella is short, along with bilateral alar hooding and a wide, bulbous, deprojected nasal tip.




The distance between the lateral maxillary segments and the central premaxilla is used to rate the severity or width of the cleft. Greater than 1 cm can be considered “wide,” often necessitating a more involved presurgical preparatory phase. This includes lip taping, presurgical NAM, staged lip procedures, delayed surgical intervention, or, in the worst-case scenarios, a premaxillary vomer osteotomy.
There is a large variability in the size of the prolabium in patients with bilateral clefts, which some hypothesize is related to the blood supply of the isolated premaxillary/prolabial segment. Even with an adequately sized prolabium, poor outcomes in lip repair can occur with designs that ignore borders of aesthetic units and subunit princi ples ( Fig. 5.8 ). The surgeon seeks to create a philtral column that is tall enough to be perceived as in the normal range after full growth. In a diminutive prolabium (< 6 mm of vertical height in prolabium; Fig. 5.5c ),27 the available prolabial skin height can be much shorter than the age-specific anthropometric normal.28
Originally described by Johanson and Ohlsson in 1960, lip adhesion has been used to narrow the alveolar cleft, reduce cleft severity for a second stage repair, and result in increased thickness of orbicularis oris (as measured by ultrasound) after the adhesion.2,29 A bilateral cleft lip adhesion can increase the size of the prolabium, making the definitive surgery much easier18 ( Fig. 5.9 ). Lip adhesions are typically performed bilaterally at 1 to 3 months of age with the definitive surgery occurring 3 to 4 months later, allowing the lip adhesion scar to mature to facilitate definitive lip repair. In patients with significant asymmetry of the bilateral cleft lip, NAM or a unilateral or bilateral lip adhesion aids greatly. The lip adhesion technique is as described in Chapter 4 for the unilateral cleft lip performed bilaterally.

Surgical Treatment Timeline
General anesthesia candidacy for the neonate with cleft lip includes adequate weight gain, lack of airway obstruction, and workup of cardiac or other abnormalities. The surgeon and pediatrician must also consider cardiopulmonary congenital deformities that could lead to failure to thrive. In 1969, Wilhelmesen and Musgrave introduced the heuristic of the “rule of 10s” as a suggestion for the appropriate timing for cleft lip repair, which included 10 weeks of age, 10 dg/mL of hemoglobin, and 10 pounds.30 Some cleft teams and surgeons prefer to repair the lip as early as the first month of life to delaying for 3 to 6 months. After birth the infant will lose weight (≤ 10% of birth weight), but this weight should be regained within 2 weeks. Adequate nutrition is noted with approximately 1 ounce of weight gain per day.
The typical timeline for each of the discrete steps of BCLP treatment is similar to that shown in Chapter 4. The bilateral cleft lip is repaired at 3 to 5 months of age, with delay allowing for both presurgical preparations (e.g., NAM) and growth to limit the nasal obstruction typically seen after bilateral lip repair. Bilateral myringotomy and tympanostomy tube placement is recommended in children with cleft palate, but systematic reviews have failed to demonstrate evidence for appropriate timing or indications.31 The authors currently place pressure equalization tubes at the primary lip repair or at the palatoplasty based on results from the tympanogram and otomicroscopy. A behavioral audiogram can be completed after 8 months of age. Speech-language pathology assessment and therapy is instituted in the first 2 years (see Chapter 11).
Secondary speech surgery may be required at 3 to 5 years of age based on speech evaluation and nasopharyngoscopy results (see Chapters 12, 13, and 14). Orthodontic consults are performed prior to the eruption of the maxillary canines (around 7 to 10 years old) to prepare for alveolar bone grafting (see Chapter 9). Orthognathic surgery for correction of dentofacial malocclusion is performed as indicated only after full skeletal growth in as many as 40% of cases in some surgeons’ experience.27 The definitive cleft septorhinoplasty is delayed until after orthognathic surgery and after full skeletal maturity (see Chapter 10).
Support for one- or two-stage bilateral cleft lip/nose repair and the timing of the primary rhinoplasty differ between institutions. In a recent review of 40 years of experience, Salyer supports the one-stage bilateral cleft lip/nose repair performed at 3 months of age for cases of complete, symmetric bilateral cleft lips.27 A two-stage lip closure is suggested in cases of asymmetric or incomplete bilateral clefts, or an “extremely small prolabium (< 6 mm in vertical height), or a displaced or severely projected premaxilla.”27 This two-stage preference is supported by Marsh and others, who perform an early bilateral lip adhesion and then definitive lip repair (Manchester-type) at 6 to 8 months.16,17 In the most severe premaxillary protrusion, early surgical premaxillary setback can be justified.17,32
Presurgical Preparation
A wide cleft lip (often ≥ 1 cm from the lateral lip to the prolabium) benefits from presurgical preparations that can include (1) lip taping ( Fig. 5.10 ), (2) an active presurgical infant orthopedic (PSIO) intraoral appliance (e.g., Latham device), (3) passive PSIO such as NAM ( Fig. 5.11 ), (4) a two-staged repair starting with a cleft lip adhesion procedure,18 or (5) in extreme cases, premaxillary vomerian osteotomy. Daily lip taping expands the soft tissue and applies orthopedic pressure to the premaxilla. The lip edges are apposed with a Steri-Strip (3M, St. Paul, MN) or tape applied to the cheeks, which are protected with skin protectant or DuoDERM sheets (ConvaTec, Princeton, NJ) ( Fig. 5.10b ). Concerns with the potential negative impact of presurgical premaxillary positioning on maxillary growth continue to fuel the debate regarding the appropriate use of PSIO.33,34

The lip adhesion technique brings the prolabial and lateral lip segments, mucosa, and lip skin together without dissection of orbicularis oris muscle, and a second definite stage is completed months later. Perlyn et al. advocate the routine use of lip adhesion to narrow a wide bilateral cleft lip, application of orthopedic pressure to the maxillary and premaxillary arches, and diminishing the wound tension at the definitive repair months later.17 The Dutchcleft Inter-center Studies found no significant benefits from PSIO in long-term maxillary arch relationships in unilateral clefts, but had not included the nasal molding aspect of NAM.35
In normal craniofacial development, the intact lip applies pressure to the premaxilla. This helps maintain the normal alveolar arch shape. Other tissues stretch to accommodate the underlying bony anatomy. This gives a normal length to the columella. In a patient with a complete BCLP, the premaxilla is anteriorly projected and the columella is not adequate (typically quite short). Additionally, the lack of blood supply from the superior labial artery may result in a smaller, diminutive prolabium.
Premaxillary Setback: The Rare Indication
Most patients with significant anterior displacement of the premaxilla require a combination of the following options: PSIO (with or without NAM),13,14 a lip adhesion procedure,18 or a delayed versus staged surgical repair.17 In severely wide cleft lip in which the child has been un-repaired and presents at 2 to 10 years of age (e.g., cases where the child presents late, which is more common now due to international adoption), PSIO may not be effective due to the maturation of the premaxillary-vomerine bony suture. Premaxillary protrusion in these cases is wrought with possible long-term side effects, most importantly midface growth disturbance. If the lip repair or adhesion is under too much tension, dehiscence will ensue ( Fig. 5.12 ).
Retropositioning of the premaxilla can be accomplished in these extreme situations with premaxillary vomer osteotomy and setback ( Fig. 5.13 ). Nasal osteotome is placed between elevated septal mucosal flaps to cut vomer. A clamp is used to conservatively remove vomer setback of the premaxilla, which is then fixated with sutures, wires, or orthodontic brackets. Significant growth inhibition is suspected after a premaxillary setback procedure,36 but stabilization of the premaxillary segment with simultaneous bone grafting, dental wires, orthodontic brackets, or permanent sutures may assist in stabilizing the segment during healing.37 The most feared complication would be devascularization of the premaxilla and slough, again warning against the routine use of premaxillary osteotomy.2 Historically, the excision of the premaxilla was performed to allow lip closure, but with awful dentofacial effects, and is unacceptable.38
Aburezq et al., in suggesting that the ideal time for premaxillary setback is at the time of the alveolar bone graft, state that “premaxillary osteotomy should be timed to coincide with a secondary (mixed dentition) bone graft, based on the stage of root development of the permanent maxillary canines.”32 This does not account for those younger children with severely projected premaxillary segments that will not move with traditional presurgical infant orthopedics. Once the osteotomy is completed, the premaxilla must by splinted or wired into position for about 5 to 6 weeks. Using interdental wires or orthodontic brackets, the premaxilla can be stabilized to the lateral maxillary arches. Aburezq et al. fabricate a dental splint that is “wired onto the orthodontic appliances in the lateral segments, and the premaxilla was seated and was held into the splint with 28-gauge wire.”32 Simultaneous alveolar bone grafting from the iliac crest is performed. In infants without dental eruption, wires can be placed around the premaxilla and lightly secured to the lateral maxillary arches. Aburezq et al. state that the contraindications to premaxillary setback include (1) mucosal scarring from incisions from previous surgery, which could impair vascularity; (2) presence of a locked-out premaxilla by constricted maxillary arches, which should first be orthodontically expanded; (3) inability to create a postoperative splint (failure to fixate the premaxilla will impair bony union); and (4) inadequate dental eruption that would limit premaxillary fixation with brackets or interdental wires.32


A clinical test that can help a surgeon determine whether a patient may require presurgical management before lip repair is a simple pinch test. In the clinic, by pinching both lateral segments of the lip together toward the prolabium, one can determine whether closure can be reached without a great deal of tension. If you cannot bring the lateral segments to reach the prolabium, then creation of a concentric orbicularis muscle will be difficult ( Fig. 5.14 ). The Manchester bilateral cleft lip repair only brings the orbicularis oris muscle edges to the lateral prolabium, but leaves a philtrum without muscular continuity.16 On the other hand, if the lateral segments reach the prolabium easily, one should expect, intraoperatively, the lip segments to move more easily. In general, the authors prefer presurgical NAM to a lip adhesion, due to the latter requiring an anesthetic and potential lip scar tissue, which might make the definitive repair more difficult.
Greyson and Cutting introduced and developed the principles of NAM (see Chapter 2), which includes the addition of nasal prongs to the traditional intraoral alveolar molding device.13,14,39 NAM will bring the maxillary alveolar segments into contact with the premaxilla. Further objectives of NAM techniques are to bring the cleft lip closer together, expand the columella mucosa and skin, and improve the nasal tip symmetry. The alveolar segments can be repositioned to come in contact prior to lip closure, allowing potential closure of the alveolar cleft with a gingivoperiosteoplasty (see Chapter 6).40
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


