Fig. 1
Pre-operative weight bearing photograph obtained during maximum ankle dorsiflexion showing right ankle equinus deformity with compensated genu recurvatum

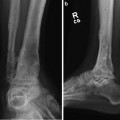
Fig. 2
Pre-operative anteroposterior-view radiograph revealing ankle arthritis . Note the joint space narrowing

Fig. 3
Pre-operative lateral-view radiograph revealing right ankle arthritis. Note the anterior osteophytes of the ankle and subtalar joint arthritis
3 Preoperative Problem List
(a)
Ankle arthritis .
(b)
Anterior ankle osteophytes.
(c)
Equinus (osseous vs. soft tissue), perform the anterior osteophyte resection then reassess the equinus to see if the posterior muscle group needs lengthening.
4 Treatment Strategy
The indications for ankle distraction are congruent joint surfaces, pain, joint mobility, and moderate to severe arthritis. Joint distraction reduces the mechanical stress on the cartilage by using an external fixation device and provides an interval healing of the cartilage surfaces.
Realignment of the soft tissue and bone is as critical to joint preservation as the joint distraction technique to obtain maximum benefits. Therefore, I utilize adjunctive procedures combined with hinged joint distraction to maximize ankle joint preservation which includes osseous realignment, soft-tissue rebalancing, and resection of osteophytes/loose bodies as required. Procedures such as core decompression, micro-fracture of osteochondral lesions, intra-articular injection of human growth hormone , and nerve decompression are also utilized when necessary.
5 Basic Principles
Joint distraction (ligamentotaxis) with external fixation for a 3-month period reduces joint loading and provides an environment in which the joint cartilage can recover. Studies have confirmed that fibrocartilage forms to restore the arthritic joint surface during distraction treatment (Salter et al. 1980, Lamm and Gourdine-Shaw 2009, van Valburg et al. 1995). Joint distraction also produces a decreased thickness of the subchondral bone, which is beneficial to increase the resiliency of the entire joint cartilage and fibrocartilage overlying the subchondral bone. Hinged ankle joint distraction with external fixation allows range-of-motion exercises and weight bearing (intermittent hydrostatic joint loading) during treatment, which increases the synovial fluid and thus provides healing of the joint cartilage.
The goals of ankle joint distraction with external fixation are to decrease pain and improve function. Joint pain is diminished by the formation of fibrocartilage, which adequately seals the cartilaginous cavity to the subchondral bone cyst and therefore eliminates increased fluid pressure and pain (Paley et al. 2008). The formation of fibrocartilage is the reason why ankle distraction leads to lasting pain relief of osteoarthritis of the ankle joint. Joint distraction typically will not improve the amount of joint range of motion but more importantly can alter the arc of motion. The arc of ankle joint motion can be adjusted based on the amount of ankle dorsiflexion planned into the hinged ankle distraction, thereby creating a more functional ankle joint without increasing the amount of joint range of motion.
6 Images During Treatment
See Figs. 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, and 14.


 8: Femoral Bone Defect
8: Femoral Bone Defect
 11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
 22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
 39: Ilizarov Ankle Fusion
39: Ilizarov Ankle Fusion
 63: Residual Clubfoot: Equinovarus Deformity/Knee Valgus/Limb Length Discrepancy
63: Residual Clubfoot: Equinovarus Deformity/Knee Valgus/Limb Length Discrepancy
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov




Fig. 4
Intra-operative fluoroscopic lateral view revealing the use of osteotomes to deepen the neck of the talus. The two osteotomes serve as a guide for resection. Note that the ankle is maximally dorsiflexed to match the portion of tibia resected. Care must be taken not to resect too much talar bone because doing so could lead to fracture, and care must be taken to resect the minimal amount of tibia to prevent subluxation of the ankle joint
Fig. 5
Intra-operative photograph revealing the use of the two osteotomes to deepen the neck of the talus with the foot in maximum dorsiflexion. The surgeon’s hand is stabilized on the foot to prevent osteotome plunging
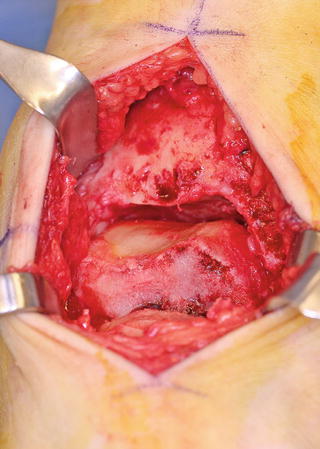
Fig. 6
Intra-operative photograph showing exposure of the joint after deepening the neck of the talus and removing residual osteophytes from the tibia with bone wax embedded into the resected bone
Related posts:
8: Femoral Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
39: Ilizarov Ankle Fusion
63: Residual Clubfoot: Equinovarus Deformity/Knee Valgus/Limb Length Discrepancy
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
