Fig. 1
A 49 year old female patient with a failed revisional total ankle arthroplasty after failure of initial ankle joint replacement which had been performed to treat post-traumatic talar avascular necrosis. Pre-operative anteroposterior view clinical photograph of a patient with a failed total ankle joint replacement. Note the limb length discrepancy and varus deformity of the foot and ankle

Fig. 2
Pre-operative lateral view clinical photograph of a patient with a failed total ankle joint replacement. Note the custom-molded brace and shoe which were required. She was in pain and unhappy with this brace

Fig. 3
Pre-operative hindfoot alignment view radiograph of a patient with a failed total ankle joint replacement. Note the subluxation and subsidence of the talar component

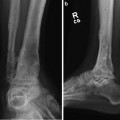
Fig. 4
Pre-operative anteroposterior view radiograph of a patient with a failed total ankle joint replacement. Note retained malaligned and subluxed talar component

Fig. 5
Pre-operative lateral view radiograph of a patient with a failed total ankle joint replacement
3 Preoperative Problem List
Failed total ankle replacement
Bone loss
Compromised subtalar joint
3-cm limb-length discrepancy
4 Treatment Strategy
Management of failed total ankle replacements can be difficult because of the complexities that lead to failure (infection, subsidence, limb length discrepancy, previous surgery, quality of bone) dictate the choice of procedure. Failed total ankle joint replacement converted to an ankle joint fusion with tibial lengthening is optimal for bone loss associated with three centimeters or less of shortening. Failed total ankle joint replacement converted to an ankle joint fusion with bone transport is optimal for bone loss greater than three centimeters associated with severe infection.
In this patient, a large segmental defect was created after removal of the implant, resulting from two failed attempts at ankle replacement. Marked LLD resulted because there was a significant bone loss after debridement to healthy bone and removal of the prosthesis. Thus, the presence of substantial bone loss and malalignment combined with the possibility of infection limits the surgical options. Circular external fixation is ideally suited to treat such a patient population. The proximal portion of the frame can be used for the purpose of lengthening, while the distal portion of the frame allows for hindfoot fusion. Because the Taylor Spatial Frame (TSF) (Smith & Nephew, Memphis, TN) is dynamic in nature, hindfoot alignment can be adjusted relative to the tibia, yielding near anatomic alignment.
5 Basic Principles
An increase in implantation of total ankle joints to treat ankle arthritis has led to a new arena of surgical treatment for the failed total ankle joint replacement. Revision total ankle joint replacement poses a significant reconstructive challenge even in the absence of infection (Nunley et al. 2012). The need for revision (removal of the prosthetic and debridement to healthy bone, reimplantation, and/or ankle fusion) leads to significant bone loss and shortening and is commonly related to failure of the talar component (Kitaoka 1991
 8: Femoral Bone Defect
8: Femoral Bone Defect
 11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
 22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
 39: Ilizarov Ankle Fusion
39: Ilizarov Ankle Fusion
 84: Lapidus Fusion with External Fixation
84: Lapidus Fusion with External Fixation
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov




Related posts:
8: Femoral Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
39: Ilizarov Ankle Fusion
84: Lapidus Fusion with External Fixation
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
