Fig. 1
Pre-operative standing radiograph showing LLD of 3.5 cm

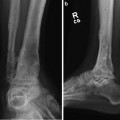
Fig. 2
Pre-operative lateral radiograph showing collapse of talar component
3 Preoperative Problem List
1.
Failed TAR
2.
Additional LLD of 3.5 cm
3.
Total bone loss expected is = LLD + bone defect after removal of TAR
4.
High suspicion of infection
4 Treatment Strategy
1.
Remove TAR and use Ilizarov/TSF to close defect with acute and gradual shortening.
2.
Take cultures at surgery to rule out infection. Hold pre-operative antibiotics to get reliable cultures.
3.
Staged surgery (4–6 weeks later) to lengthen the tibia. Bone defect of 5 cm after removal of TAR is anticipated. Total bone loss is equal to LLD (3.5 cm) + bone defect after TAR removal (5 cm) = 8.5 cm.
4.
Use LATN technique to shorten time in frame.
5 Basic Principles
1.
Excise TAR through medial and lateral incisions.
2.
Acute plus gradual shortening of bone defect with TSF.
3.
Avoid bone graft in setting of infection.
4.
Acute shortening of more than 3 cm is inadvisable. This will make wound closure difficult and can adversely affect neurovascular status.
5.
Check pulses during surgery to make sure you are not acutely shortening too much.
6.
Total bone loss is preexisting LLD plus bone defect from removal of TAR.
7.
LATN shortens time in frame by substituting an intramedullary nail during the consolidation phase. The rod is inserted before the frame is removed. There is no contact between internal and external fixation. The proximal tibial external fixation is placed peripherally in the bone out of the path of the intramedullary rod.
6 Images During Treatment
See Figs. 3, 4, 5, 6, 7, 8, 9, 10, and 11
 8: Femoral Bone Defect
8: Femoral Bone Defect
 11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
 22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
 39: Ilizarov Ankle Fusion
39: Ilizarov Ankle Fusion
 84: Lapidus Fusion with External Fixation
84: Lapidus Fusion with External Fixation
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov




Related posts:
8: Femoral Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
39: Ilizarov Ankle Fusion
84: Lapidus Fusion with External Fixation
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
