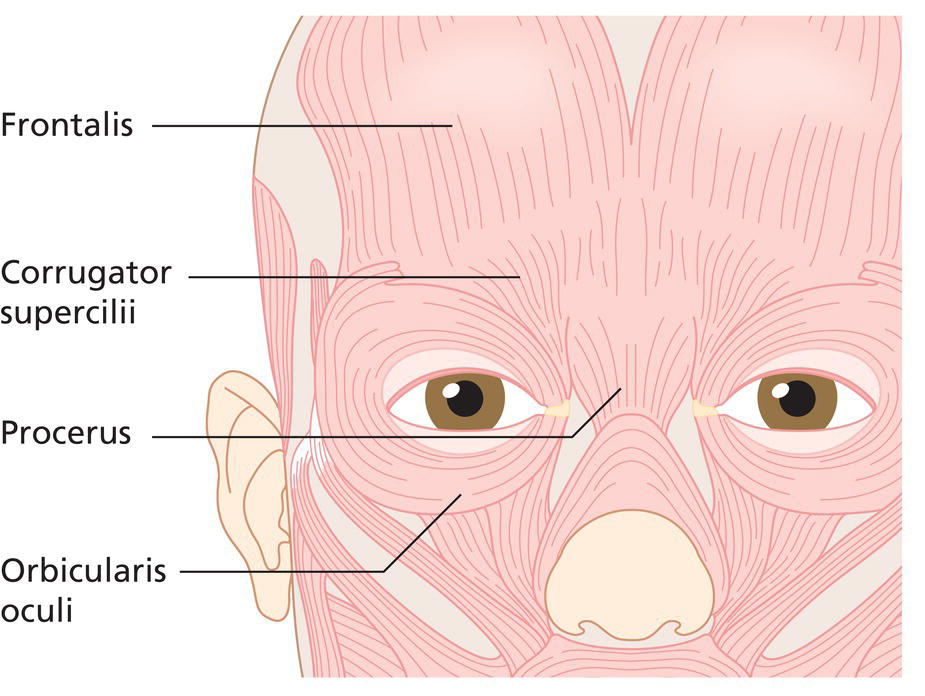
Margit L.W. Juhasz1, Scott R. Freeman2, and Joel L. Cohen1,3 1 University of California, Irvine, CA, USA 2 Sunrise Dermatology, Mobile, AL, USA 3 AboutSkin Dermatology and DermSurgery, Greenwood Village, CO, USA Botulinum toxins are produced by the Gram‐positive, spore‐forming anaerobe Clostridium botulinum, and cause chemical denervation by suppressing the release of the neurotransmitter acetylcholine from the axon terminals of peripheral nerves. There are seven distinct subtypes of botulinum toxin (A–G), with types A and B being the only clinically relevant subtypes at this time. Currently, there are four botulinum neurotoxin type A (BoNTA) and one botulinum neurotoxin B (BoNTB) toxins available for human use in the United States. Botox® (onabotulinumtoxinA, Allergan, Inc., Irvine, CA, USA), Dysport® (abobotulinumtoxinA, Medicis Pharmaceuticals Corp., Scottsdale, AZ, USA), Xeomin® (incobotulinumtoxinA, Merz, Frankfurt, Germany), Jeuveau™ (prabotulinumtoxinA‐xvfs, Evolus, Newport Beach, CA, United States) comprise the four type A toxins currently available. Botox is currently US Food and Drug Administration (FDA) approved for several non‐cosmetic therapeutic indications (including blepharospasm, strabismus, and axillary hyperhidrosis), as well as for cosmetic use for temporary improvement of moderate to severe glabellar lines (approved 2002) and lateral canthal rhytides/crow’s feet (2013). Dysport is FDA approved for treatment of cervical dystonia and has cosmetic indication for temporary improvement of moderate to severe glabellar frown lines (2009). Xeomin is FDA indicated for treatment of cervical dystonia and blepharospasm, as well as for temporary improvement of moderate to severe glabellar frown lines (2011). Jeuveau, the newest to market type A toxin in the United States, is approved for temporary improvement of moderate to severe glabella frown lines (2019). Myobloc® (Rimabotulinum toxin, Solstice Pharmaceuticals, South San Francisco, CA, USA), a type B botulinum toxin, is currently only approved for the therapeutic treatment of cervical dystonia (2000). While the various type A botulinum toxins are FDA approved for cosmetic use in the glabella (all) and crow’s feet (Botox only), they are used off‐label in various other facial sites as well. Additionally, while Botox is also FDA approved for axillary hyperhidrosis, Botox as well as Dysport and Xeomin are also used off‐label for hyperhidrosis of the palms, soles, face, and scalp. PrabotulinumtoxinA (JeuveauTM and Nabota® [Daewoong Pharmaceuticals, Seoul, South Korea]) has been used off‐label for the treatment of periorbital rhytides, contouring of calves and myofascial pain syndrome [1–3]. Treatment doses are not interchangeable between botulinum products (even among the strains of type A toxin) and all references to BoNTA dose, unless otherwise stated in this chapter, refer to and are specific for Botox. Clostridial bacteria secrete high molecular weight protein complexes that include three key proteins: a 150‐kDa toxin, a non‐toxin hemagglutinin protein, and a non‐toxin non‐hemagglutinin protein. The non‐toxin proteins may provide the toxin complex protection against temperature or enzymatic denaturation [4], or at least that has been a historical perspective by some of the formulators. The 150‐kDa toxin is cleaved by bacterial proteases to form a di‐chain composed of a 100‐kDa heavy chain and a 50‐kDa light chain. Disulfide and non‐covalent bonds link the heavy and light chains, and both chains are required for neurotoxicity [4]. In 1987, Canadian ophthalmologist Jean Carruthers recognized the cosmetic potential of BoNTA. While treating patients for benign essential blepharospasm, Dr. Carruthers noted that several patients treated for blepharospasm had significant improvement of dynamic rhytides in the periocular region. Following this observation, the husband and wife team of Drs. Alastair and Jean Carruthers began more systematic studies of BoNTA for cosmetic indications. In 1991, the Carruthers reported their initial findings of cosmetic treatment with BoNTA at North American dermatology and ophthalmology meetings. After initiating clinical trials, their first publication on this topic was in 1992, demonstrating the safe and effective treatment of dynamic rhytides in the glabella with BoNTA [5]. After over a decade of off‐label cosmetic use in the United States, BoNTA (Botox) was approved specifically for the treatment of glabellar rhytides in 2002. Currently, off‐label cosmetic uses continue to expand with regions of treatment encompassing not only the forehead and periocular areas, but also the mid‐face, lower face, neck, and décolleté. Botox and other BoNTA toxins are also widely used worldwide for medical and therapeutic purposes, including the treatment of hyperhidrosis, headaches, spasticity disorders, and depression. This chapter highlights both traditional and newer cosmetic applications of BoNTA. The process of chemical denervation requires that the neurotoxin heavy chain bind the synaptic vesicle glycoprotein 2 (SV2) on the presynaptic nerve terminal. This process leads to toxin–receptor complex endocytosis with subsequent toxin light chain release through vesicle lysis [6]. All toxins cause chemical denervation by suppressing the release of acetylcholine from the axon terminals of peripheral motor nerves. After vesicle lysis occurs within the axon terminus, toxin light chains ultimately prevent neurotransmission by cleaving specific protein isoforms necessary for the docking, fusion, and release of acetylcholine from this nerve terminus. Toxins A, C, and E cleave synaptosomal‐associated protein 25 (SNAP‐25) and toxins B, D, F, and G cleave vesicle associated membrane protein (VAMP, also known as synaptobrevin) [4]. Muscle paralysis typically occurs within approximately 3–7 days, and synaptic regeneration reverses the paralytic effect within 3–6 months [6]. The neurotoxin–protein complex size of Botox is approximately 900 kDa and the most common vial size used is 100 units, though it is available in 50 units as well. One vial contains 5 ng of toxin. One unit (U) is standardized to equal the median amount necessary to kill 50% of female Swiss‐Webster mice after intraperitoneal injection (LD50) [6–8]. Botox is a vacuum‐dried product, and in addition to 100 U of toxin, each vial contains 500 μg albumin and 900 μg sodium chloride [4, 8]. Typical cosmetic doses of Botox range from 10 to 60 units, depending on the number of areas treated in one session. The complex size of Dysport ranges from 500 to 900 kDa, and one vial contains 300 units of freeze‐dried abobotulinum toxin. In addition, each 300 unit vial contains 125 μg of human serum albumin and 2.5 mg lactose. Xeomin is a vacuum‐dried 150 kDa toxin protein free from biologically inert complexing proteins. Xeomin is packaged in 50 and 100 unit vials, and in addition to the active toxin, each 100 unit vial also contains 1 mg human serum albumin and 4.7 mg sucrose [9]. Each single‐dose vial of Jeuveau contains 100 units of vacuum‐dried powder prabotulinumtoxinA‐xvfs, 500 mg of human serum albumin, and 900 mg of sodium chloride [10]. Product characteristics of Botox compared with the other FDA‐approved neurotoxins are provided in Table 44.1. Package inserts indicate that Botox, Dysport, and Jeuveau should be stored at 2–8°C and away from light. Xeomin is stable at room temperature (20–25 °C), but may also be stored at refrigerator (2–8°C) or freezer (−20 to −10°C) temperatures for up to 36 months. Once a vial of Botox, Xeomin, or Jeuveau has been reconstituted, product should be stored at 2–8°C and should be used within 24 hours. Dysport, once reconstituted, should be stored at 2–8°C and administered within 4 hours. However, recent studies suggest that botulinum toxin products product may be viable for much longer when properly handled. A double‐blind, randomized study of 30 patients showed no significant difference in the treatment of canthal lines between those treated with Botox reconstituted with sterile, non‐preserved saline immediately prior to injection compared with toxin reconstituted 1 week prior to injection [12]. Furthermore, another study demonstrated that Botox reconstitution at times ranging 1–6 weeks prior to injection produced statistically similar results in patients treated for glabellar rhytides compared with product reconstitution 1 day prior to injection [13]. While none of these three agents should be shaken, they are often lightly swirled upon reconstitution – and it is recommended that Xeomin actually be inverted to most effectively reconstitute the product. Table 44.1 Botulinum toxin comparison.a a Dosages are not equivalent between products. b Food and Drug Administration. c Allergan, Inc., Irvine, CA, USA. d Medicis, Scottsdale, AZ, USA. e Merz, Frankfurt, Germany. f Evolus, Newport Beach, CA, USA. g Solstice Pharmaceuticals, South San Francisco, CA, USA. Marketed as Neurobloc outside of the USA. h Synaptosomal‐associated protein 25 (SNAP‐25). i Vesicle‐associated membrane protein (synaptobrevin). Botulinum toxinA has a large margin of safety, with an estimated human median lethal dose of 1.3–2.1 ng/kg when injected intramuscularly or intravenously. This correlates to a LD50 of approximately 26–42 U/kg, making its cosmetic use a relatively safe endeavor at recommended cosmetic doses [14, 15]. Care should be taken to use the necessary dosing ranges in a given region in order to optimize patient satisfaction and preserve a natural result. Injectors should possess excellent knowledge of facial anatomy, especially considering the close proximity of adjacent musculature that may not be part of the intended area of treatment. Contraindications to BoNTA are few and are listed in Table 44.2 along with several medications that require caution when administering BoNTA [16]. Prior to treatment, patients should be informed that the typical duration of glabellar efficacy for all BoNTA is likely to be 3–4 months. Potential side effects should be discussed. Duration studies comparing the duration of efficacy for the various type A toxins have yielded mixed results and it is not clear which toxin, if any, has the most long‐lasting effect. The mean onset of action for BoNTA should also be discussed with the patient, as some patients may have misperceptions and expect immediate results. While it has been published that Dysport onset often starts by Day 1, a recent Botox study demonstrated that approximately half of patients experience initial onset by postinjection day 1 and nearly all patients will experience onset of action by day 4 [17]. Table 44.2 Precautions and contraindications. Informed consents should clearly indicate that treatment of areas other than those approved by the FDA constitute off‐label use. Consent should be in the form of an oral discussion as well as a signed, written document. Pretreatment asymmetries and scars should always be discussed, documented, and we also recommend photography prior to treatment. Patient satisfaction may be improved by the application of ice packs to the intended treatment areas prior to injection of toxin. This serves a twofold purpose by providing mild anesthesia to the treatment area as well as causing vasoconstriction, thereby potentially decreasing the risk of bruising. While we provide suggested doses (herein listed in Botox units) for various injection techniques, it must be remembered that these should serve as guidelines for the practitioner and not as a “cookbook.” Treatment doses should be patient specific and be primarily based on prominence of individual muscles as well as patient preference. For example, the corrugator supercilii of the typical male patient are larger and more prominent than those of the average female. Additional consideration for the patient’s desired result should be made and addressed during the pretreatment interview, as some patients prefer little to no movement in the treated muscles, while others may prefer a gentle softening of movement of treated area. The forehead, for example, is an area where it is very important to discuss this difference with patients. Additionally, we caution against attempts to apply “conversion factors” to equate Botox, Dysport, Xeomin, and Jeuveau. While they may provide a general guide for the beginner, we recommend that that the injector becomes familiar with the use and properties of each neuromodulator agent they choose to employ in their practice. Photodamage and overactive musculature can cause changes in the upper face that convey a fatigued or angry look that is often discordant with reality. Treatment of the upper face with BoNTA can lead to a more youthful, relaxed, and rested appearance [18, 19]. Data also support the use of BoNTA in multiple areas of the upper face in a single treatment session [20]. The frontalis muscle is contiguous with the galea aponeurotica of the scalp superiorly, and inserts inferiorly into the skin of the brow. Its configuration varies between individuals but it is generally considered to be either a uniform band across the forehead or V‐shaped with a relative absence of fibers medially (Figure 44.1). Fibers of the frontalis are oriented vertically, and thus when they contract the brows elevate and horizontal forehead lines become imprinted in the skin over time. The lateral fibers of the orbicularis oculi muscle pull down on the lateral brow, and thus directly oppose the upward forces of the frontalis. This muscular interaction allows for the creation of a neurotoxin lateral brow lift (discussed below). Figure 44.1 Relevant musculature of the upper face. (Source: Sommer B, Sattler G, eds. (2001) Botulinum Toxin in Aesthetic Medicine. Blackwell Science, Boston, MA. Reproduced with permission of John Wiley & Sons.) A recent Botox consensus article addressed treatment of horizontal forehead lines caused by the frontalis [21]. The authors recommended ranges of 6–15 U and 6 to <15 U BoNTA for females and males, respectively (Table 44.3), and agreed that doses over 20 U are more likely to lead to complications or patient dissatisfaction (e.g. eyebrow ptosis and patient complaints of immobility and unnatural appearance). Forehead injections of BoNTA are generally placed over 4–9 injection sites. In order to avoid eyebrow ptosis, the injections should generally not be placed any closer than 1–1.5 cm above the bony orbital rim (Figure 44.2). Patients with tall foreheads may benefit from 2 to 3 rows of injections, and patients with wider foreheads may also require more injection sites. Attention to the shape and positioning of the patients baseline brow is essential, and often injection sites in women are performed in an arch to try to preserve the arch of the brow below. Patients with dermatochalasis or low‐set brows should be evaluated carefully prior to injection as they represent the population most at risk for significant eyebrow ptosis and/or complaints of “heaviness” after treatment. Accordingly, older patients who are more dependent upon their frontalis for brow elevation will typically not tolerate (or at least not like) the higher doses that younger patients will tolerate, and thus are most frequently treated with lower doses. Patients with significant etched‐in lines immediately superior to their lateral brows are also patients who may frequently be advised not to have BoNTA treatment as they depend on the baseline action of the lower frontalis fibers to hoist the brow upward and away from their eyelid. These patients may benefit from other treatments including tightening devices, lifting devices, filler agents to occupy volume, or surgical correction with brow lift techniques. Table 44.3 Treatment recommendations by site (Botox units).
CHAPTER 44
Botulinum Toxins
Introduction
Mechanism of action
Neurotoxin physical characteristics
Product stability
Botox c
Dysport d
Xeomin e
Jeuveau f
Myobloc g
Serotype
A
A
A
A
B
Molecular weight (kDa)
900
300–500
150
900
700
FDAb approved for cosmetic use?
Yes
Yes
Yes
Yes
No
Total clostridial protein weight per vial (ng)
5j
4.35j
0.6j
3.75
25, 50, or 100
Units per vial
100
500
100
100
5000
pH (after reconstitution)
5.6
5.6
5.6
5.6
5.6
Target
SNAP‐25h
SNAP‐25
SNAP‐25
SNAP‐25
VAMPi
Safety and contraindications
Standard injection techniques
General considerations
Precaution
Mechanism
Cyclosporine
Has been reported to cause neuromuscular blockade, possibly through calcium channel blockade
Aminoglycoside antibiotics
Large doses can prevent release of acetylcholine from neurons
D‐penicillamine
May cause formation of antibodies targeting acetylcholine receptor
Contraindication
Myasthenia gravis
Autoantibodies targeting acetylcholine receptor
Lambert–Eaton syndrome
Paraneoplastic, antibodies targeting calcium channels
Amyotrophic lateral sclerosis
Neurodegenerative disease
Pregnancy or breastfeeding
Insufficient safety data
Allergy to any constituent of BoNTA
Potential for anaphylaxis
Treatment of the upper face
Forehead
Treatment site
Muscles
Typical number of injection points
Typical total Botox units a
Women
Men
Upper face
Horizontal forehead lines
Frontalis
4–9
6–15
6 to >15
Glabellar complex
Procerus, depressor supercilii, orbicularis oculi
5–7
10–30
20–40
Crow’s feet
Orbicularis oculi
2–4 per side
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access