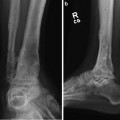
Fig. 1
The talus is ripped from the multiple capsular connections with the tibia plafond and calcaneus. There is often complex fracturing of the talus. The talar body is extruded through the soft tissue envelope

Fig. 2
Loss of the talar body as a result of the trauma. The open fracture is debrided and the ankle joint is supported by half-pin distraction frame. Antibiotic beads are placed in the bone defect
3 Preoperative Problem List
1.
There are complex wounds associated with open ejection injuries of the talus. There may be areas of skin necrosis that develop over the first week following the injury. Because of severe swelling the wounds cannot be closed.
2.
These injuries are often associated with midfoot fractures and open wounds.
3.
Loss of the talar body will result in 3–4 cm of shortening of the extremity if the calcaneus is fused to the tibia plafond.
4.
The entire talus may be lost to the injury with no talar head fragment.
5.
Injuries to the posterior tibial nerve and artery may be associated with open talus fractures.
4 Treatment Strategy
The initial complex decision is between reconstructing the talus with internal fixation and discarding the talar fragments and salvaging the extremity with tibia-calcaneal arthrodesis. The soft tissue condition and the level of contamination will determine if the arthrodesis is attempted with internal fixation and allograft augmentation or reconstruction with Ilizarov method using external fixation and proximal bone transport. The Ilizarov method is also indicated when there has been failure of internal fixation of talus fractures with nonunion and infection.
5 Basic Principles
1.
The traumatic wound requires aggressive debridement removing all necrotic soft tissue and bone. Infected nonunions require aggressive debridement, identification of the infecting organism, and intravenous antibiotics.
2.
Bridging external fixation is applied to resuscitate the zone of injury. The reconstruction is delayed for 10–21 days to allow recovery of the soft tissue envelope.
3.
The alignment of the arthrodesis is determined by the presence of a viable talar head or complete loss of the talus. Reconstructing the ankle with the talar head in place allows improved forefoot motion which occurs through the talar navicular and calcaneal cuboid joints. Always salvage the talar head if it is viable.
4.
Proximal lengthening of the tibia is elective. If the patient has medical comorbidities or psychological issues, a 3 cm shoe lift can be used to equalize leg length.
6 Images During Treatment
See Figs. 3, 4, 5, 6, 7, 8, 9
 8: Femoral Bone Defect
8: Femoral Bone Defect
 11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
 22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
 39: Ilizarov Ankle Fusion
39: Ilizarov Ankle Fusion
 84: Lapidus Fusion with External Fixation
84: Lapidus Fusion with External Fixation
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov




Related posts:
8: Femoral Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
39: Ilizarov Ankle Fusion
84: Lapidus Fusion with External Fixation
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
