4. Facial Aging
4.1 Introduction
Evolution, a story of progressive adaptation and development, is mirrored in the sea change that has occurred in both our understanding and our management of facial aging. In Darwin’s time, “naysayers” and adherents of the conventional wisdom refused to accept the new way of comprehending the development of the world and its inhabitants. Ideas were being challenged in a manner that required a rethinking of well-worn theories. In plastic surgery, a simplistic approach of tightening that which has sagged has given way to a yet-to-be-completed exploration of both the cause and treatment of facial aging.
4.2 What Has Changed?
Our understanding of the aging process has shifted from one that is gravity-centric to one whose foundation is volume-centric. Advances in understanding the anatomy of the face have been combined with an insightful analysis of the internal facial dynamics that are reflected in external signs of aging. This intellectual and academic synergy has enabled us to offer more effective surgical solutions to our patients. It has also led to the burgeoning realm of nonsurgical treatments that are designed to be compatible with our current concept of facial aging via the injection of volumizing fillers.
This chapter consolidates current facial aging theories and research to provide a foundation on which to offer treatments that meet the expectations of our patients and those of ourselves.
4.3 Characteristic Stigmata of Facial Aging
The variation in treatment options we may offer to patients in the same age category is a testament to the lack of uniformity seen in facial aging. Multiple anatomical, genetic, and environmental factors can affect the onset of any of the well-known stigmata of facial aging. Critical analysis of the patient enables a thoughtful treatment plan that is tailored to the specific needs of the individual.
4.3.1 Temporal Hollow and Brow Ptosis
The loss of a youthful fullness in the temple results in a concavity that is associated with aging of the upper third of the face (Fig. 4.1). It is frequently accompanied by descent of the tail of the brow that produces a visual contrast of excess (brow ptosis) and deficiency (temporal hollow).
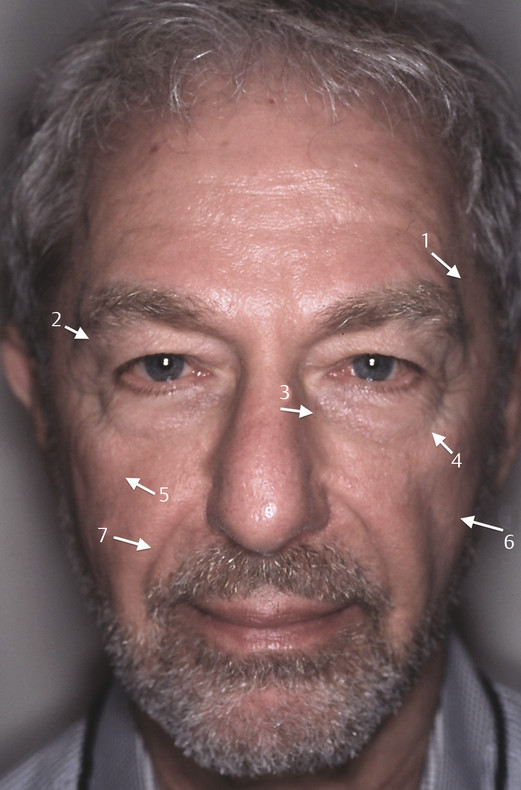
4.3.2 Tear Trough and Lid–Cheek Junction
The tear trough is produced by the tear–trough ligament and extends in an oblique direction to the midpupillary line from the medial canthus (Fig. 4.1). As it migrates laterally with age, the tear trough frequently joins the lid–cheek junction or palpebromalar groove formed by the orbicularis retaining ligament (Fig. 4.1). 1 , 2 , 3 The continuous groove thus created produces a distinct visual boundary between the orbital fat and the midcheek. 4 , 5
4.3.3 Malar Bag
A combination of sagging and anterior bulging of the prezygomatic space that is formed by the orbicularis and zygomatic retaining ligaments produces the distinctive baggy appearance overlying the malar bone (Fig. 4.1). 2
4.3.4 Cheek Flattening
The joining of a convex and a concave curve known as the ogee is an architectural analogy that has provided a visual symbol for the various theories of facial aging. Little has noted it to be emblematic of youth, and its decline in aging is a by-product of additive and subtractive volume-related changes in the face. 6 Flattening of the convexity of the ogee that descends from the cheek to the lower face accompanies the diminished facial volume of aging (Fig. 4.1).
4.3.5 Nasolabial Crease
The crease lies medial to the nasolabial fat compartment (nasolabial fold) that is bounded laterally by the medial compartment of the malar fat. The onset and depth of the crease represent an interplay of deep midfacial fat volume depletion and apparent compartment addition that is symbolic of many of the aging changes that occur in the face. 7 It has been described as a manifestation of pseudoptosis (Fig. 4.1). 8
4.3.6 Jowl
Formation of the jowl is considered a confluence of fixed ligaments and mobile fat interactions at the anterior mandible and masseteric border. 9 Attenuation of the mandibular septum enables the jowl fat compartments to descend with a clear demarcation of the anterior jowl produced by the mandibular ligament (Fig. 4.2). In cadaver dissections, Reece et al9 observed distinct superior and inferior subcutaneous fat compartments above the mandibular border with the anterior boundary of the superior compartment noted to be the oral commissure and the inferior fat compartment positioned more posteriorly. They are separated from a single fat compartment below the mandibular border by the mandibular septum, which they described as a sling. Of note, fibers of the platysma were seen to accompany the septum to its insertion 1 cm superior to the mandibular border.
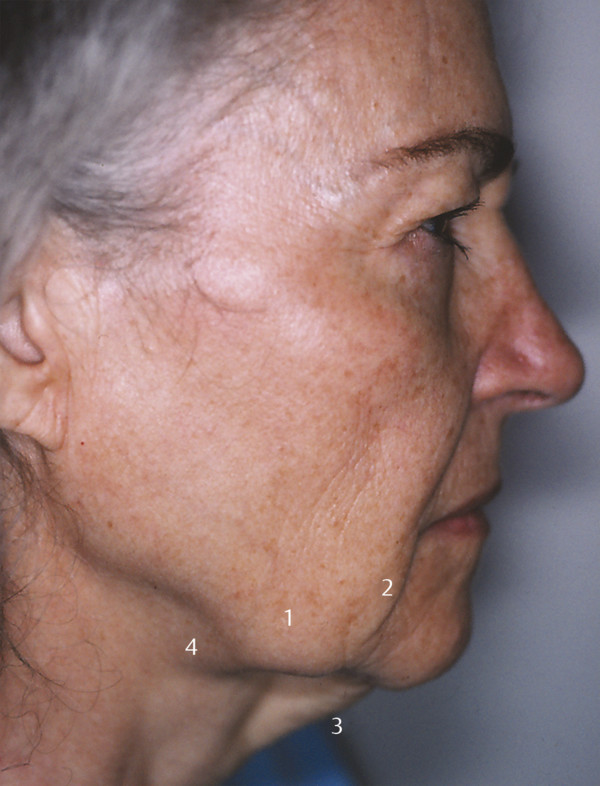
4.3.7 Marionette Line
The visible line in front of the jowl that creates a visual demarcation between the mandible and chin often appears as an inferior extension of the nasolabial fold (Fig. 4.2).
4.3.8 Neck Sagging
The aging changes that occur in the neck result from alterations in the skin, fat, muscle, and bone components. These changes convert the acute cervicomental angle of youth to an oblique angle often accompanied by a loss of mandibular border definition. Ellenbogen and Karlin described the optimum cervicomental angle as ranging from 102 to 110 degrees. 10 In addition, they discussed the importance of a well-defined mandibular border, a subhyoid depression, and visibility of the thyroid cartilage and the anterior sternocleidomastoid border in the appearance of a youthful neck. Whereas laxity and redundancy of skin are present to varying degrees in the aging neck, the accompanying changes in fat, muscle, and bone have a significant impact on neck contour and must be considered in the evaluation of the patient.
As described by Stuzin, the close approximation of the platysma muscle to the deep cervical fascia in youth is the result of retaining ligaments. 11 A variable decussation pattern is present, the most common being a joining of the medial platysmal borders for only 1 to 2 cm below the chin. 12 According to Stuzin, loss of support for the platysma occurs when the retaining ligaments weaken. Inferior descent of the muscle with the development of banding of the anterior border of the platysma and conversion to an oblique neck contour are by-products of this loss of support, along with age-related hypertrophy of the muscle (Fig. 4.2). Lambros believes the aging changes seen in the platysma are due to bowstringing of the muscle rather than muscle descent (personal communication, 2014).
Similar to the face, the neck has defined fat compartments that affect its appearance. The submental fat, subplatysmal fat, and deep fat compartments must all be considered when analyzing the aging neck. A limited study of 10 cadavers by Larson et al found most neck fat to be located in the supraplatysmal (44.7%) and subplatysmal (30.7%) compartments. 13 Rohrich and Pessa described three distinct subplatysmal fat compartments. 14 The central subfascial fat is bordered by a medial compartment superficial to the mylohyoid muscle and a lateral compartment located lateral to the anterior digastric muscle.
Two additional elements that contribute to the aesthetic appearance of the neck are the digastric muscles and the submandibular gland. The significance of their contribution to the contour of the neck can be obscured by overlying skin and fat but may be evident in the postoperative patient if not recognized and addressed during surgery. The bulk present in the anterior belly of the digastric muscle can add to submental fullness and contributes to the lack of a distinct mandibular border in the aging neck. 15 Increased visibility of the submandibular gland with prominence of the superficial lobe located lateral to the digastric muscle causes an additional disruptive convexity below the border of the mandible (Fig. 4.2). Whether this is true submandibular gland ptosis or pseudoptosis, as postulated by Raveendran et al, requires further investigation. 16 Finally, changes in the dimensions and volume of the mandible can diminish the defined mandibular border associated with a youthful appearance. 17
4.4 Components of Facial Aging
Developing a treatment plan for addressing the stigmata of aging requires a multifaceted understanding of the components that contribute to the outward appearance of the face.
4.4.1 Fat: Volume Distribution versus Volume Loss
The traditional concept of a cohesive volume of facial fat that responds to gravity and the aging process in a uniform manner has undergone great scrutiny in the past decade. Gravity in the aging process is best understood as having a differential impact based on the degree of support provided by the structural fat compartments and bony contours of the face. The volumetric differences evident in the spectrum of aging seen within each age cohort counter any efforts at quantifying the impact of gravity. Current thinking on the effect of aging on facial fat tends to stratify into altered volume distribution versus volume loss. These two theories can be considered compatible rather than divergent.
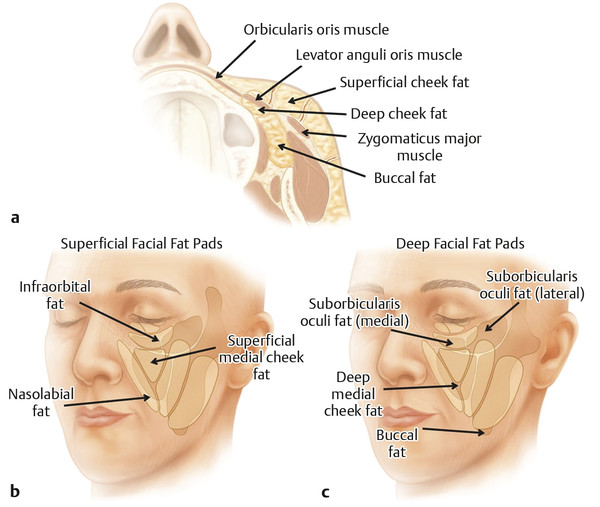
Rohrich and Pessa showed in their dye partition studies that the various anatomical units of subcutaneous fat in the face, known as compartments, are segregated by septa. These fibrous condensations of connective tissue extend from the superficial fascial layer to the dermis. 7 , 18 Four distinct cheek fat compartments were found that they named the nasolabial fat compartment, the medial cheek fat compartment, the middle cheek fat compartment, and the lateral temporal–cheek compartment. Each compartment has a variable response to aging, and a treatment plan needs to consider both the amount of fat that remains in each compartment and its position. They postulated that the lack of success in reducing the prominence of the nasolabial fold with lateral traction of the skin and fat can be explained by the compartmentalization of the nasolabial fold fat. In addition, they described a deep midfacial fat compartment medial to the zygomaticus major muscle and stressed the significance of an age-related decline in fat volume in this location. 8 Its proximity to the superficial medial cheek fat compartment suggests the potential role of a diminished deep midfacial fat compartment in the loss of midface projection attributable to a lack of structural support (Fig. 4.3).
An effort was made to understand the aging changes seen in the facial fat compartments by using computed tomography scanning in a study performed by Gierloff et al. 19 Many of the observations made in the dye partition studies were confirmed using their methods. In particular, sagittal-diameter measurements of the deep medial cheek fat were consistent with both a decrease in volume and an inferior shift of fat associated with aging. They found evidence of volume loss in the buccal extension of the buccal fat pad and posited this loss to be a contributor to the appearance of the tear trough. Although their data were not conclusive from their data, they theorized that the lack of buccal extension support results in a descent of the medial and middle cheek fat compartments and thereby deepens the lid–cheek junction.
The loss of midface projection has the secondary effect of interrupting the youthful continuity of the cheek, thereby isolating the nasolabial fold fat compartment and making it appear more prominent. Proponents of volume loss through fat atrophy, termed facial deflation by Lambros, 20 consider age-related changes in the amount of facial fat to be a major contributor to the appearance of the aging face. The lack of descent of skin landmarks with stability of the lid–cheek junction, as documented in serial photographs, was interpreted by Lambros as being consistent with the central role of volume loss as opposed to sagging in facial aging. He has observed that the deflation associated with aging manifests in a more directional, lateral to medial, than compartmental sequence (personal communication, 2014). A cellular study by Wan et al compared the deep with the superficial midfacial fat compartments in an elderly cadaver population. This study showed adipocytes that were significantly smaller in the deep medial cheek compartment compared with those in the superficial nasolabial fat compartment and suggested an accelerated rate of deflation in the deep compared with the superficial fat. 21 This finding would lend credence to the concept of facial deflation that occurs selectively with a resultant pseudoptosis of the superficial fat resulting from a volumetric decline in deep compartment support. 8
Some advocates of aging as the by-product of altered volume distribution in the face adhere to the concept of segmented zones of facial fat that shift as the relationship between the soft tissue spaces and the retaining ligaments changes over time. Wong and Mendelson have described a series of bulges and troughs that partition the midcheek into the lid–cheek, malar, and nasolabial components. 22 They emphasized that the troughs that appear are the result of the fixed retaining ligaments that have come to be defined externally by the mobility of the intervening soft tissue spaces: the preseptal, prezygomatic, and premaxillary. This external mapping of the soft tissue spaces is a distinctive feature of the aging face.
Stuzin et al attribute the change in volume distribution in the face to a progressive laxity that occurs in the retaining ligaments. 23 In this concept, the structural supportive function of the ligaments declines and the fat descends as a consequence. Stuzin also described a radial expansion of the soft tissue of the face as the result of an age-related weakening of the retinacular fiber attachments between skin, fat, and deep fascia that he believes produces an outward prolapse from the bony skeleton. 11 Reece et al have linked changes in the mandibular septum to the onset of jowls. 9
Many authors have come to the conclusion that a combination of facial fat descent, attenuation of retaining ligaments, and diminished volume produces the characteristic stigmata of the aging face. Open questions remain as to the role and significance of skeletal aging in the changes that occur in the facial fat compartments over time. The primary or secondary cause of many of the aging changes seen clinically has yet to be elucidated. As our understanding of facial fat compartments has expanded, there is an inherent risk in compartmentalizing our analysis and treatment. We need to consider not only the aging-induced changes that occur in a particular fat compartment but also the impact that those changes may have on adjacent regions of the face. Similarly, an algorithm that incorporates the compartmentalization concept into a proposed treatment plan must also anticipate the consequences that treating each compartment may have on other anatomical compartments and ultimately on the outward appearance of the face.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


