4 Cleft Lip Repair: Unilateral
Introduction
Cleft lip and cleft palate are the most common birth defects of craniofacial development. Up to 7,000 children with a cleft are born each year in the United States.1 The surgical repair of the cleft lip deformity only skims the surface of the comprehensive management programs that interdisciplinary cleft teams provide for these children. The American Cleft Palate Association guidelines suggest a team of specialists that may include anesthesiology, audiology, radiology, genetics/dysmorphology, neurosurgery, nursing, ophthalmology, oral and maxillofacial surgery, orthodontics, otolaryngology-head and neck surgery, pediatrics, pediatric dentistry, physical anthropology, plastic surgery, prosthodontics, psychiatry, psychology, social work, and speech-language pathology.2 Certainly, not every team will involve all of these specialties. The team′s effectiveness as individual providers is magnified when collaborative discussion of care expands the knowledge base of the group. The team will diagnose and treat cleft-related and coexisting conditions, which range from genetic analysis, hearing and speech, dental and orthodontic, bone grafting, and orthognathic surgery.
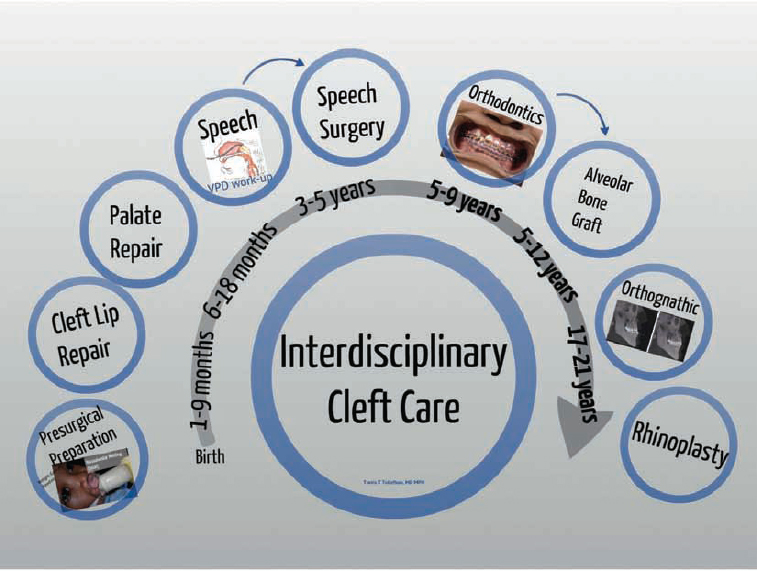
A schematic of the treatment plan for a child born with cleft lip can be organized as a timeline, beginning prenatally and extending into the late teenage years and early adulthood ( Fig. 4.1 ). Each aspect of the authors’ treatment management algorithm should be presented and supported by the best available levels of evidence. The clinical decision points in the treatment algorithm are examined using the principles of evidence-based medicine.3 Cleft lip repair techniques are emphasized in this chapter, beginning with a historical perspective and leading to the authors’ preferred methods. This chapter also outlines cleft classifications, epidemiology, interdisciplinary care concepts, physical exam findings, preoperative preparation for the lip repair, and postoperative management protocols.
Historical Perspective
Many cite the first cleft lip repair documentation from China in 390 AD4; others credit Celsus with a lip repair description in the first century.5 Ambroise Pare, the 16th-century French barber-surgeon, proclaimed that surgery is “to eliminate that which is superfluous, restore that which has been dislocated, separate that which has been united, join that which has been divided and repair the defects of nature.”6 In 1564, he described paring the cleft lip margins and then skewering the raw edges with needles, while using a figure-of-eight-type linen or silk suture to wrap around the needle.
By 1844, the first flap techniques were described by Mirault, who rotated a lateral lip segment across to the medial lip.7 Essentially, the three schools of cleft lip repair design include the straight line closure, geometric, and rotation-advancement techniques. Many modifications have been blended from these general categories, but the progression of ideas is worth discussing. As Mark Twain wrote, “there is no such thing as a new idea. It is impossible. We simply take a lot of old ideas and put them into a sort of mental kaleidoscope. We give them a turn and they make new and curious combinations. We keep on turning and making new combinations indefinitely; but they are the same old pieces of colored glass that have been in use through all the ages.”8
Surgical innovations were only one improvement in cleft lip repair. Surgeons were afforded a safer environment and additional time for surgical repairs with the advent of modern anesthesia techniques, more refined surgical instruments, and creation of delicate suture materials.9
Straight Line Designs
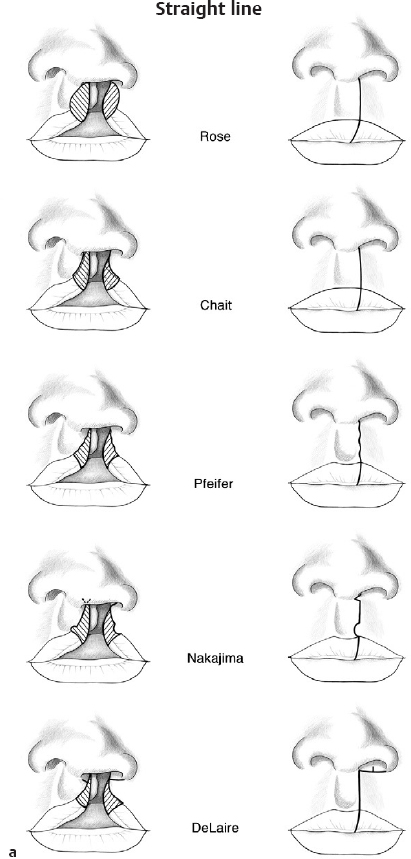
The first straight line closures were first described by Rose in 1881, which included paired incision designs that extended from the nasal floor to the vermilion border ( Fig. 4.2a ).10 Layered wound closure with catgut and wire was introduced. Thompson′s modifications were described in 191211 and are referred to as Rose Thompson.12 In a recent U.S. survey of 269 North American cleft teams, Demke and Tatum found that only 1% of contemporary surgeons used the strict straight line technique.9 Straight line cleft lip repair has had additional modifications, which include the Delaire technique (1975). A laterally based triangle to be inset into a backcut at the top of the medial cleft is needed to obtain the adequate lip height. The Delaire cleft lip principles are best known for emphasis on wide subperiosteal undermining with a theoretical perioral musculature repositioning.13
Geometric Designs
In 1955, LeMesurier reintroduced the geometric lip repair technique based on Hagedorn′s description of a laterally based quadrangular lip flap ( Fig. 4.2b ).14 The Tennison flap repair,15 which included a triangular flap from the inferior part of the lateral lip, was modified by Randall in 1959 and remains commonly used.16,17 Tennison′s novel use of a bent wire stencil was instrumental in the shift to mathematical accuracy of the flap designs.18 In 1958, Skoog employed two smaller triangles from the lateral lip, which produce extra lip length. These triangles were inset at the base of the columella and at the vermilion-cutaneous junction.19 In the Demke-Tatum survey, only 9% described using the triangular flap technique in unilateral cleft lip repair. These were subdivided into the Fisher subunit technique (28%), Randall-Tennison technique (48%), Nakajima technique (4%), and Davies Z-plasty technique (12%).9
Rotation-Advancement Design
A paradigm shift was described in 1955 when Ralph Millard described the rotation-advancement technique that he developed during military service in the Korean War ( Fig. 4.2c ).20,21 The crux of the design is curved line on the noncleft (medial) side lip, which was intended to address the lip height discrepancy between the medial and lateral cleft sides.22 A curvilinear line was designed on the noncleft side, which unfurled to give more lip height. A more symmetric lip height, philtral column width, and nasal base symmetry were planned.23
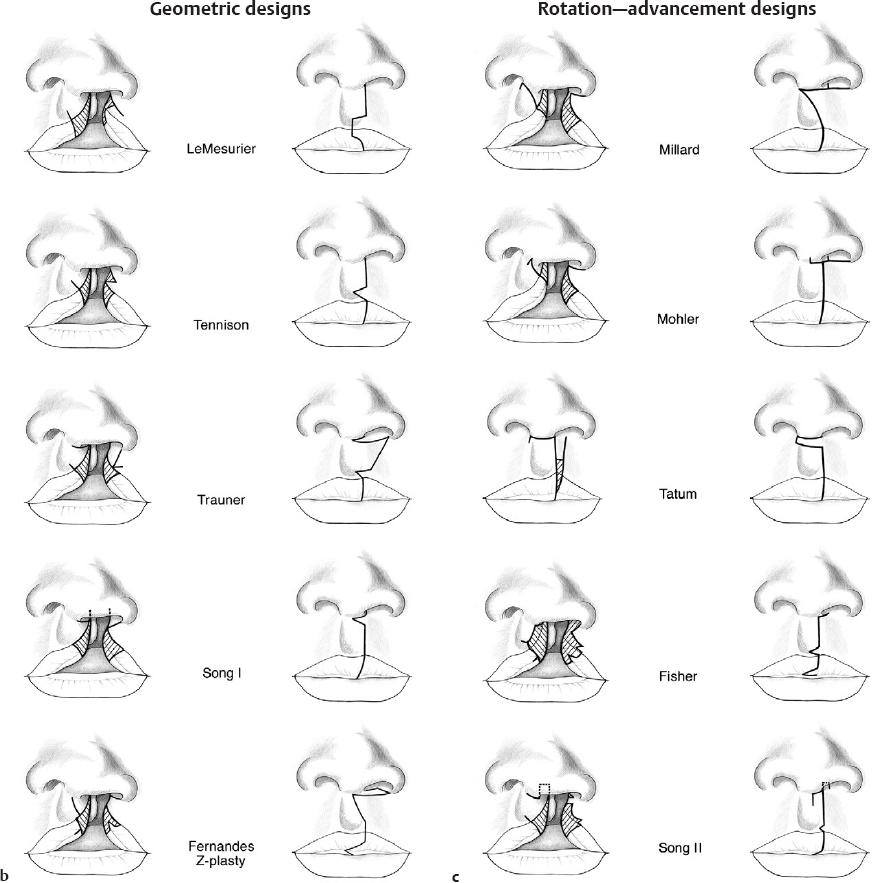
In 1987, Mohler described one of the most effective modifications of the Millard technique.24 The columellar flap (c-flap) was rotated into the columella instead of rotating laterally into a back cut at the alar base. The rotational flap incision extended into the columella, which borrows columellar skin to lengthen the lip. With the c-flap rotated into the columella, the cleft-side nostril is not narrowed. Cutting et al. found that the extended Mohler modification was successful at preventing a short lip.25,26
The most popular contemporary techniques are the Millard, Mohler modification, and the triangular flap designs. In the previously mentioned survey, 46% of U.S. surgeons primarily use the Millard repair, whereas an additional 38% use a modification of the rotation-advancement technique.9
Noordhoff defined the “red line” in the lip at the junction of the dry and wet vermilion ( Fig. 4.3 ).27 Careful scrutiny of this area will consistently show that the medial dry vermilion tapers out as it courses superiorly into the cleft margin. This is a key area that many novice surgeons neglect. Noordhoff used a laterally based triangle formed from the dry lip mucosa on the lateral lip and inset just below the dry lip mucosa on the medial lip. He further modified the rotation-advancement technique with a second triangle. A precisely designed laterally based triangle flap was inset into the medial cutaneous roll to achieve additional vertically lengthening of the medial lip.27,28
Surgical Principles
In 1938, Dr. Victor Veau presented a fundamental principle regarding the reconstruction of the muscle layer. First, the basis of the repair is the release and repair of the muscle layers. Second, he emphasized the repair of the nasal floor and sill after creating a foundation with underlying musculature. Further, like others, he advocated the preservation of the cleft tissue during the repair. We strongly agree with conserving as much tissue as possible.29
With these principles, the aberrant orbicularis oris muscles are widely undermined from the cleft lip edges. The nasal base attachments to the maxilla are released in a subperiosteal plane allowing less tension on the orbicularis oris closure. The nasal floor is released in a submucoperiosteal plane and closed. The nasal floor repair is strengthened with a layered closure of the orbicularis and perinasal muscles that have been released from the anterior nasal spine periosteum. The aberrant orbicularis oris fiber insertion sites on the noncleft side of the anterior nasal spine often deform the typically midline structure to the noncleft side, along with the caudal septum. On the contrary, some surgeons warn that secondary facial growth inhibition may be exacerbated by these principles of more extensive undermining.
Classification
Orofacial clefts include the typical cleft lip with and without cleft palate. This abnormal opening of the lip, nasal sill, alveolus, and palate can occur in a spectrum of combinations of unilateral or bilateral deformities. The etiology of orofacial clefting is poorly understood, but occurs as a defect in the complex pathways of craniofacial developmental as described in Chapter 1. Cleft lip and palate can occur as complete or incomplete clefts, depending on the structures involved. The nomenclature for diminutive expressions of orofacial clefts includes the terms microform, occult, minor, or forme frust (aborted form).29
A variety of classification schemes have been suggested over the last decades, but the Veau classification has endured since 1938. Veau described group A as including defects of the soft palate alone. Group B demonstrates hard and soft palate defects, but not extending anterior to the incisive foramen. Group C involves unilateral cleft lip defects extending through the entire palate and through the alveolus. Group D includes complete bilateral cleft lip.29 The simplicity of this categorization is useful for discussion between providers and comparisons. With increasing understanding of the aberrant developmental pathways responsible for oro-facial clefts, the schema for classification has expanded to more specific anatomic structures.

Proper classification is imperative for targeted treatment guided by a comprehensive cleft management algorithm. The involvement of the primary and secondary palate—with special attention to the lip and nasal deformity—is assessed less than complete cleft features. First, determine if the cleft is typical or atypical. The atypical craniofacial clefts were classically described by Paul Tessier in 1976, who described the classification scheme for orofacial clefts that present with atypical orientation. This cleft taxonomy involves a numbering system that describes which structures of the craniofacial soft tissue and skeleton are involved in the cleft. For example, a Tessier No. 7 cleft includes macrostomia due to a cleft at the commissure of the lip ( Fig. 4.4 ).30 These craniofacial clefts can extend to the maxilla, orbit, and skull base. Similar to the typical clefts, a spectrum of severity is possible.
The features of a typical orofacial cleft that begin the classification process include the following:
Laterality (left, right, asymmetric/symmetric bilateral)
Classification from complete ( Fig. 4.3 ), incomplete ( Fig. 4.5 ), or microform ( Fig. 4.6 )
Severity of width
Presence or absence of abnormal tissue (e.g., Simonart bands) (see Fig. 5.6b)

The cleft lip laterality is noted, but occasional bilateral cleft palate is found with unilateral cleft lip. The cleft alveolus can be complete or notched. Independent of the cleft lip type, the cleft palate is described as unilateral (one palatal shelf is attached to the nasal septum) or bilateral.
The complete cleft lip extends through the lip and nasal sill. An incomplete cleft is often defined as including the orbicularis oris and skin, but with some intact lip tissue. An often-argued aspect is the presence of a Simonart band at the base of the nasal sill. The Simonart band is a weblike tissue extending from the cleft to the noncleft side at the nasal sill. This is not universally considered the same as an incomplete cleft, which often includes mesenchymal elements (orbicularis oris and follicular glands).
Veau described the microform cleft lip as the forme fruste (meaning aborted form), but the theory that the cleft partially “healed” in the womb was soon disproven. Mulliken characterized the microform cleft lip with the following: (1) a philtral skin groove, (2) minor nasal deformity, (3) orbicularis oris discontinuity, and (4) a notched vermilion-cutaneous junction with disruption extending to no more than a quarter of the labial height, measured from the normal peak of the upper lip junction between the white and red lip (Cupid bow) to the nasal sill.31
Epidemiology
Orofacial clefting is a heterogeneous set of defects with a significant variability in severity and occurrence rates. It is the most commonly occurring congenital/developmental craniofacial anomaly, but it ranks fourth amongst the most common overall birth defects (after congenital heart deformities, spina bifida, and limb deformities). The incidence rates for orofacial clefts differ based on geography, ethnicity, and gender. The distinct differences in the occurrence of cleft lip and palate are demonstrated by a higher incidence in populations from Native American and Asian backgrounds and lowest in African ancestry.1
The incidence of all facial clefting in the United States has been reported to be between 1:600 and 1:750 live births.1 The quality and accuracy of the birth defect registries and databases and the estimations made by statistical modeling must be considered when interpreting these findings. There are no consistent patterns of occurrence of clefts during certain seasons, or identifiable time trends, but further investigation is warranted.32 The prevalence of cleft lip with or without cleft palate has shown recent trends of increasing prevalence in the United States (7.75 per 10,000 live births) and slightly decreasing internationally (7.94 per 10,000 live births).33
Nearly 300 associated syndromes have been related to orofacial clefting. The most common associated syndromes include velocardiofacial syndrome (an autosomal dominant 22Q11.2 deletion, with variable expressions of cardiac defects, a broad nasal root, and dysmorphology of the skull base and velopharyngeal structures), van der Woude (autosomal dominant characterized by cleft palate and lip pitting), and oculo-auriculo-vertebral syndrome, which includes Goldenhar syndrome (an autosomal dominant condition characterized by variable expressions of vertebral anomalies, ocular dermoids, hemifacial microsomia, and auricular deformities).
The etiology of cleft lip and palate is multifactorial. The exact interplay between environmental factors and genetic predisposition is not clear. Basic preventative measures for expecting mothers include prenatal multivitamins (folic acid supplementation), tobacco cessation,34 and minimizing perinatal alcohol consumption. Maternal folic acid supplementation is recommended for prevention of neural tube defects, but there is conflicting evidence of the effectiveness of protection against developing orofacial clefts. A 2010 Cochrane review of randomized controlled trials failed to link a decreased risk of cleft lip and palate when prenatal folic acid was given. An overall protective effect against neural tube defects was found.35
Interdisciplinary Care
The interdisciplinary care team should consist of some of the following: audiology, genetics, nursing, oral and maxillofacial surgery, orthodontics, otolaryngology-head and neck surgery, pediatrics, pediatric dentistry, facial plastic surgery, social work, and speech-language pathology.2 A neonate with cleft lip with or without cleft palate may have associated dysmorphic features. Typically, the pediatrician on the team will work alongside the primary care pediatrician to identify cardiac murmurs, limb deformities, and neurologic/development delay. The team geneticist thoroughly examines the neonate and makes anthropometric measurement, as well as additional chromosomal analysis. Microarray testing is often obtained. Fluorescence in situ hybridization may detect a micro-deletion of chromosome 22q11.2, indicating velocardio-facial syndrome in children when physical features are suggestive.
The hearing assessment begins with the pediatrician′s evaluation of the ears and a newborn hearing screening shortly after birth. Audiologists evaluate for congenital sensorineural or conductive hearing loss with conventional audiogram tympanograms in infancy; however, the behavioral audiograms can be obtained after 7 to 8 months of age. Questionable or inconsistent results will call for an auditory brainstem response test. All newborns with cleft lip and palate receive a screening audiogram due to the possible eustachian tube dysfunction associated with abnormal veli palatini musculature in cleft palate.
One of the roles of the otolaryngologist is to evaluate hearing and presence or absence of middle ear pathology/effusions. The routine use of tympanostomy tubes may prevent chronic ear effusions and the associated conductive hearing loss, but is currently a matter of clinical controversy. Ponduri et al. completed a systematic review of studies regarding routine compared to selective placement of tympanostomy tubes in children with cleft palate. They determined that a paucity of quality randomized controlled trials was available, but that routine placement in the neonatal period does not seem to be indicated.36 This is contradicted by the practice patterns of many cleft teams, who tend to place the first set of tympanostomy tubes at the time of the cleft lip repair.37 Further studies are needed to address this complex clinical dilemma.
Prenatal surgical consultation is now more commonly performed. Expecting mothers can present shortly after diagnosis on prenatal ultrasound. This can introduce feeding and surgical care plans to the family, which may alleviate some anxiety and empower the parents to learn about feeding strategies. Genetic counseling is informed by the rates of having a child with a cleft if one or both parents, or a direct relative, has a cleft. It is generally accepted that associated malformations occur more frequently in infants who have cleft palate than in those who have cleft lip and palate and even less still in those with isolated cleft lip. For example, a 17-year study in France reported the rate of associated malformations as 46.7% in cleft palate, 36.8% in cleft lip and palate, and 13.6% in cleft lip.38
Immediately after birth, the physician′s priorities are to assure weight gain and evaluate for concurrent cardiac or other deformities. Parents will be prepared and educated on feeding strategies, surgical repairs, and team care. The team social worker can assist with state-sponsored assistance. This exposure also allows the team members to begin determining the parental willingness to travel and cooperate with presurgical preparations like presurgical nasoalveolar molding (see Chapter 2), which necessitates frequent clinic visits and parental commitment.
The dental and maxillofacial team members include pediatric dentistry, orthodontists, and oral and maxillofacial surgeons. Early dental care on a biannual basis is advocated as to empower the child and parents to dental care. An orthodontic appointment is made around 5 to 7 years of age to allow the treatment plan for palatal expansion, tooth alignment, and preparations for an alveolar bone graft (if warranted). The oral and maxillofacial surgeon contributes additional insight into the timing and type of alveolar bone grafting, maxillary and mandibular facial growth, and suitability to surgically assisted palatal expansion. As the teenager reaches full skeletal maturity, preparations for orthognathic surgery or distraction osteogenesis procedures are addressed. Some teams address this later aspect of care with collaboration between the pediatric otolaryngology-head and neck surgeons, facial plastic and reconstructive surgeons, plastic surgeons, and oral and maxillofacial surgeons.
Examination of the Unilateral Cleft Lip/Cleft Palate
The neonate is examined for cleft lip with or without cleft palate immediately after birth. A practitioner must gain training and experience to identify the more subtle muscle abnormalities of the microform cleft lip and submucous cleft palate. The continuity of the upper lip, alveolar arches, and nostrils are palpated and inspected. The various presentations of orofacial clefting (cleft lip, alveolus, or palate) are assessed independently. The cleft is classified based on the most typical features of the uni-lateral cleft lip–cleft palate as a guide, but unique cases occur. For example, a unilateral complete cleft lip and palate may be paired with a contralateral microform cleft lip and intact alveolus, making the classification either an asymmetric bilateral cleft or a unilateral with contralateral microform.
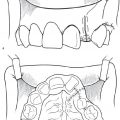
Laying the child supine in the parent′s lap and carefully extending the neck can enhance examination of the soft palate ( Fig. 4.7 ). The neonate often spontaneously opens his/her mouth and protrudes the tongue, providing a good view. When indicated, a tongue depressor and headlight are useful in watching for movement of the soft palate and a bifid uvula. A possible submucous cleft palate should be palpated with a finger to feel for a hard palate notch. The lower lips are inspected for lip pits (Van der Woude syndrome). The oral commissures, eyelids, and nostrils are inspected for atypical clefting. Examination for findings of oculo-auriculo-vertebral spectrum includes the shape and position of the ears (microtia), features of hemifacial microsomia, and eyelids with coloboma or notches.

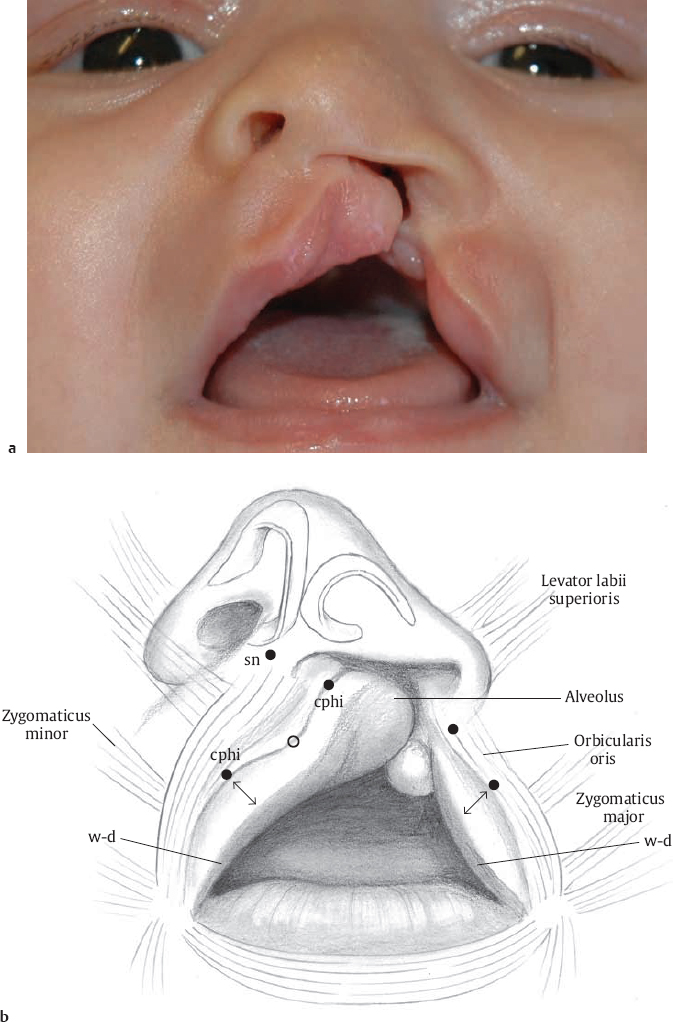
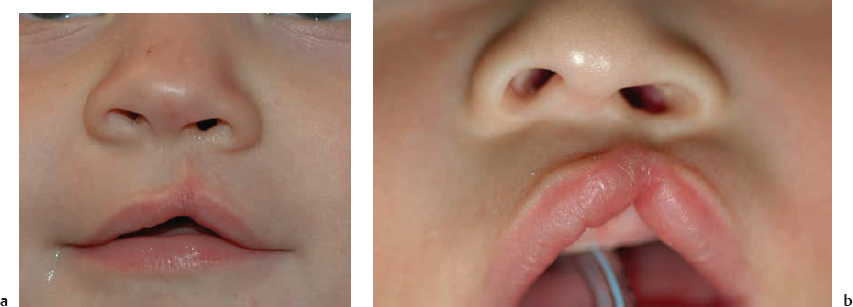
There is a wide variation in the severity of unilateral cleft lip and palate. The complete cleft lip is a separation of the lip, nasal sill, alveolus, and palate ( Fig. 4.8 ). An incomplete cleft lip extends to more than a quarter of the labial height ( Fig. 4.5 ). The casual observer can neglect to identify the dysmorphic features of a microform cleft lip ( Fig. 4.6 ). A recently termed nanoform cleft39 (also referred to as minor-microform) is the most diminutive form. The characteristics of a microform cleft lip include divot in the philtral column, absence of orbicularis oris muscle fibers throughout the height of the lip, vermilion-cutaneous notching (extending to no more than a quarter of the labial height), and a minor nasal base asymmetry with alar hooding.31
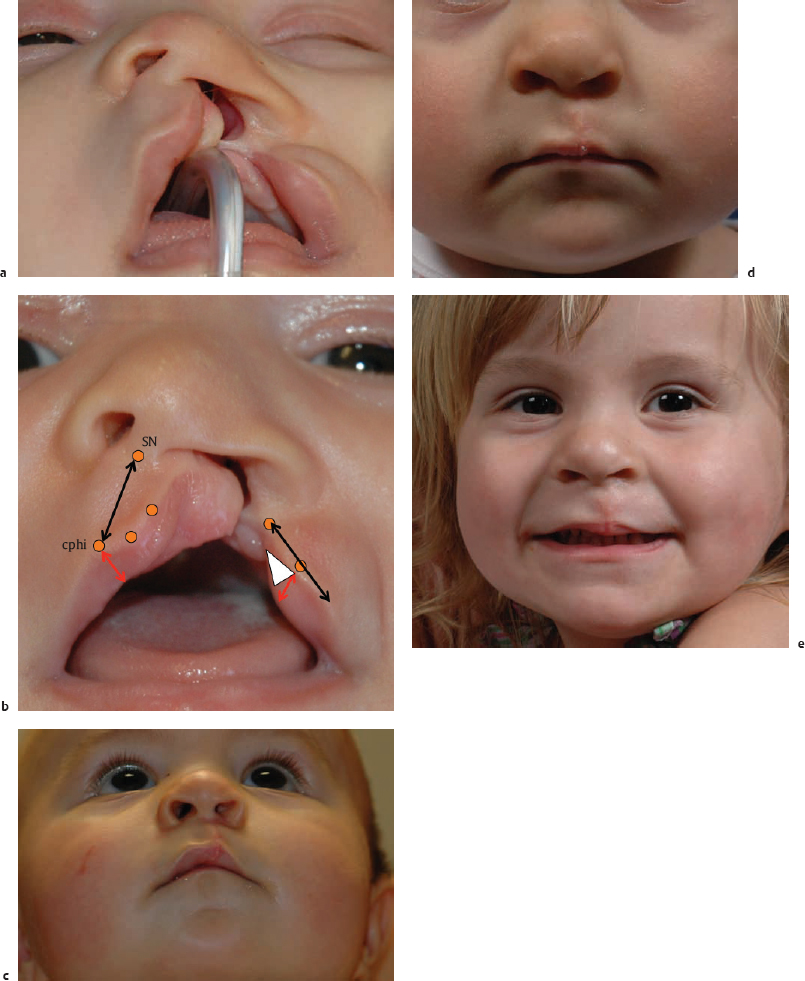
The nasal alar base on the cleft side will splay during smiling due to the aberrant orbicularis oris attachments. For purposes of consistency, the two sides of the cleft lip are defined as cleft (lateral) and noncleft (medial). The cutaneous lip vertical height on the noncleft side is short. Other characteristics to observe are the deficient dry vermilion on this medial lip ( Fig. 4.8b ) and caudal septal deflection to the noncleft side. The cleft lip nasal deformity is inspected for (1) cleft side nasal ala hooding, (2) stunted and asymmetric tip projection (secondary to dysmorphic lower lateral cartilages), and (3) alar base malposition due to both deficiency in bone (maxillary alveolar cleft) and tissue (dysmorphic/aberrantly inserted orbicularis oris and skin/mucosal deficiency).
Relevant Anatomy
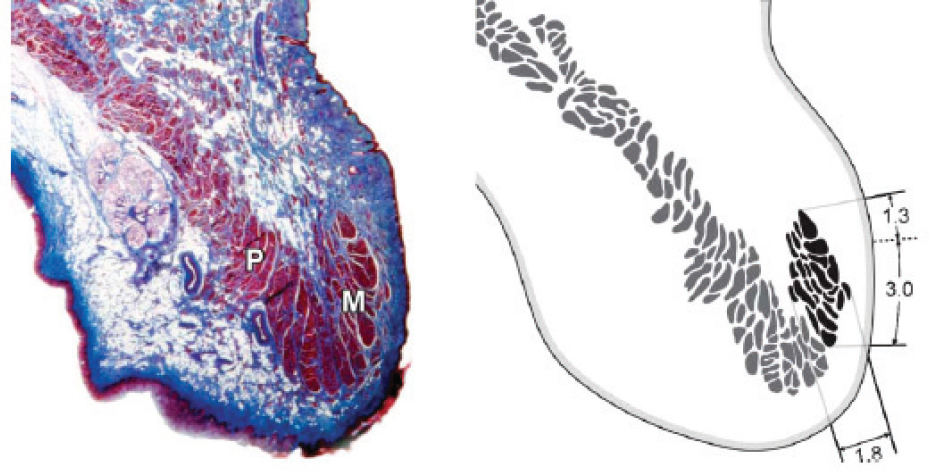
In the unilateral cleft lip deformity, the most commonly mentioned muscle is the orbicularis oris, which is a complex, circular layer of muscular fibers that is often simplified in illustrations. The pars marginalis component of the orbicularis oris is a more linear band located at the level of the cutaneous (or white) roll. The pars marginalis extends between the two commissures ( Fig. 4.9 ). When these contract, they create a greater depression superior to the phil-trum and help outline the architecture of the Cupid bow.40
The pars peripheralis is the sphincteric component of the orbicularis oris musculature. Complex lip movements are made by coordinated contractions, creating both puckering and interlabial pressure against apposed food or other structures. The facial muscles that insert around the mouth interact to create the complex motions needed to create speech and facial expressions. Some of these perioral muscles include the zygomaticus major and minor, levator labii superioris, levator alaeque nasi, risorius, and the transverse constrictor muscles of the nares (nasalis). Delaire describes these nasolabial oblique bands that extend from the nasal septum and nares down to the commissures of the lips. He described how these bands interweave with the perioral musculature. In coordination with the more horizontal bands (lip puckering), these more oblique bands protrude the lip forward as well as narrow the vestibular opening.13
The normal anatomy of the perioral musculature can be translated into the complete unilateral cleft lip. In the unilateral cleft lip deformity, a network of linear and oblique muscle components extend up to the base of the columella, nasal spine, and caudal septum. The constant contractions of these aberrant muscle fibers are hypothesized to deviate the nasal spine and caudal septum to the noncleft side in the unilateral cleft lip deformity.13 This can be seen on typical examination in these unilateral cleft deformities. The contralateral cleft side orbicularis oris and perioral musculature insert aberrantly to the base of the nose. This is easily demonstrated when observing the cry of a child with an unrepaired unilateral cleft lip. The cleft side alar base is also splayed laterally due to the aberrant muscle insertions.
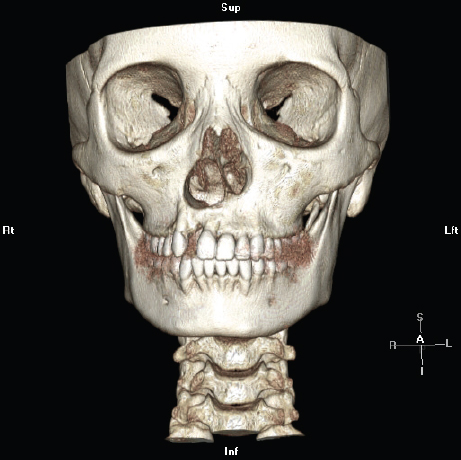
A classic description of the unrepaired unilateral cleft lip nasal deformity includes hooding or flattening of the cleft side nostril with variable severity. The cleft side alar base is typically laterally, posteriorly, and inferiorly displaced. The inferior displacement occurs secondary to the skeletal deformity, as the lateral maxillary development has also been impaired with the alveolar cleft formation ( Fig. 4.10 ).
Park et al. attempted to answer whether the cleft side nasal cartilages were hypoplastic or just deformed. During cleft lip rhinoplasty, the authors meticulously measured the width, length, and thickness of the lower lateral cartilages in 35 adult and pediatric patients with cleft lip. They compared the gross and histologic morphology of lower lateral cartilage on the cleft side to the noncleft side. The deformed cleft side cartilages had similar volumes of cartilage when compared to the noncleft side, but were distorted. The cleft side lower lateral cartilage was deformed into more linear and less curvilinear shape when compared to the noncleft lower lateral cartilage.41 The nasal tip lacks definition. Additional fibrofatty tissue is positioned between the domes of the lower lateral cartilages.
Some surgeons prefer to remove soft tissue from the lateral ala and alar base during the primary rhinoplasty. Aberrant mesenchymal remnants in the junction of the cleft side nasal ala add fullness and bulk to the nostril shape. The argument for removal of this tissue remains unanswered. The typical septal and nasal spine deviation to the noncleft side can also be addressed in that primary setting by suture suspension of the caudal septum to the midline, but the repercussions on growth are unknown.
Standard anatomic descriptions for the cleft lip deformity include those seen in Fig. 4.8 . The vermilion-cutaneous junction and wet-dry vermilion junction are essential anatomic elements to be restored during the lip repair. Landmarks can be delineated, when coursing superior to inferior, to include the subnasale at the base of the columella, philtral column extending to the cutaneous roll (often called white roll), vermilion-cutaneous junction (red-white lip junction), dry vermilion, and wet-dry vermilion junction (Noordoff′s red line). A cross-sectional histology of the upper orbicularis oris musculature demonstrates the pars peripheralis and pars marginalis differentiation ( Fig. 4.9 ).
The cleft lip repair design is based off proper anatomic identification of the junctions of normal skin to mucosa, with attention to the quality of the tissue. Hair follicles or velum are often absent in the fine hair-bearing skin at the cleft lip margins, which are often used to design the incisions. This embryologically immature skin should be left out of the lip repair, which is especially important in the male when considering facial hair growth. Mulliken clearly described the difference in the skin edges of normal versus unusable skin at the cleft margins: “Normal skin has lanugo hairs that diffuse light; there are visible glandular openings. Abnormal, hypoplastic skin is glabrous (without fine hairs), thin, and shiny (without glandular openings).”31
The surgeon must decide the layer to undermine the lip and cheek soft tissues from the maxilla, sub-, or supra-periosteal. Delaire hypothesized that supraperiosteal undermining of the soft tissue from the maxilla may adversely affect bony growth, while subperiosteal elevation (as he advocated) does not. The anatomic basis for this theory is the two-layered makeup of the periosteum: an external (fibrous) and internal (cellular) layer. The external layer supplies a rich vascular supply to the internal layer of osteoblasts. He suggested that the vascular supply of this external fibrous layer must be preserved and, therefore, denounces the supraperiosteal dissection.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


