This article examines the application of 3D fusion of postoperative anatomy superimposed upon preoperative anatomy to evaluate the changes in soft tissues relative to fixed bony structures. The value of 3D analysis is to predict and quantitatively measure the soft tissue changes associated with skeletal orthognathic surgery. An example is shown of changes in the upper lip that occur after Le Fort I osteotomy, illustrating how these soft tissue changes can be measures with the 3D software. Uses and future applications of this technology are described.
Accurate facial analysis is the cornerstone of aesthetic and functional surgery of the face. Its importance is defined by the necessity to define preoperative and postoperative goals, as a function of both surgical objectives and meeting patient desires and expectations. Simulating and defining the augmentation of soft tissue position after surgery has been a paramount objective of surgeons for more than a century, yet current methods of attaining this objective remain dated. This article discusses the use of advanced imaging technology and software analysis to objectify midface soft tissue movement in a three-dimensional (3D) model after Le Fort osteotomies and maxillary advancement. Although discussed here in the context of a single procedure, the potential applications of this method of analysis are countless.
Facial analysis is rooted in antiquity, with coordinate measurement systems being adopted in Egypt, India, Greece, and Byzantium. The renaissance brought about a more technical system of analysis, notably Leonardo da Vinci’s facial proportions. The current aesthetic ideal is a combination of patient desires, contemporary concepts of beauty, and the surgeon’s concept of beauty.
Measurement systems, based on two-dimensional (2D) analysis have been created to capture these ideals. These techniques include cephalometrics and clinical photography. The 2D model uses multiple coordinates in an attempt to capture the third dimension, which is depth. Although useful, this model limits analysis to mostly linear surgical vectors (eg, anterior-posterior dimension). Current measurements depend on soft tissue coordinates relative to fixed bony landmarks.
Present technology allows only limited analysis in 2 dimensions. For example, analysis of midface soft tissue following Le Fort osteotomies is generally performed using lateral views, which is a limited measurement technique. After midfacial advancement, the upper lip is changed in size, position, and shape. Limited 2D analysis allows us to measure the change in projection, or length of the lip in a given plane. However, the observer sees the changes in the lip in 3 dimensions, not on a single plane. Just as the human eye analyzes the entire midface after Le Fort osteotomies, so should the analysis.
3D imaging protocols have been studied for more than a decade. However, broad advancements in imaging techniques and analytical software are beginning to transfer these tools from research to clinical application. 3D imaging has the potential to largely replace standard cephalometry, in which the head film is a 2D representation of a 3D object. Cone beam computed tomography (CBCT) in combination with surface scanning allows the creation of the electronic patient, allowing the ability to create, modify, and predict surgical outcomes. This situation not only provides an opportunity for surgical planning but also creates a powerful communication interface between treating physicians and patients. This article proposes the use of 3D imaging protocols to accurately assess surgical treatment goals before and after orthognathic surgery.
Global goals in plastic surgery include visualization and measurement of presurgical simulation and outcomes of surgery. This process needs to be simple and accurate. Presurgical simulation should create a surgical objective and a blueprint for surgery. Outcomes assessment creates the opportunity to measure cause-and-effect relationships between skeletal manipulations or soft tissue augmentations and the final soft tissue results. Outcomes analyses can be used to refine the simulation and outcomes predictions.
3D modeling technique
An example of current 2D analysis is shown by lip analysis. The boundaries of the lip reside in the lower third of the face. The vertical boundaries of the upper lip are the subnasale (superiorly) and stomion superius (inferiorly), and those of the lower lip are the stomion inferius (superiorly) and menton (inferiorly). The upper lip/lower lip height ratio (Sn−Stm s /Stm i -Me′) is approximately 1:2. Holdaway describes 11 techniques for measuring soft tissue balance, which include facial angle, upper lip curvature, skeletal convexity at point A, upper lip strain and thickness, and lower sulcus depth. These parameters are measured with 2D imaging techniques, including standard 6-view photography and cephalograms. Current measurement parameters measure the change in lip position as a function of upper lip thickness and position in relation to fixed bony points.
Schendel and Lane have described image fusion techniques and their application to surgical craniofacial and dental anatomy. This article furthers this application to the evaluation of soft tissue anatomy. Image fusion is a combination of CBCT and 3D facial surface imaging (stereo photogrammetry). Stereo photogrammetry is an advanced software system applied to the fundamental technique of taking 2 or more pictures of the same object using single reflex lenses, at a distance differential similar to the distance between a pair of eyes. This process creates a composite 3D model using complex triangulation algorithms to identify and match unique surface markers. After a 3D geometric shape has been formed, the software maps color texture onto the model. Each color represents the amount the soft tissue has moved anteriorly or posteriorly in relation to a fixed bony landmark. This surface image is overlaid on the skeletal framework obtained from the CBCT scan, with the skull base used as an anchoring point. The clinician is able to use the color mapping to quickly analyze postsurgical changes. The result is the most accurate electronic representation of surgical changes to craniofacial anatomy available to date.
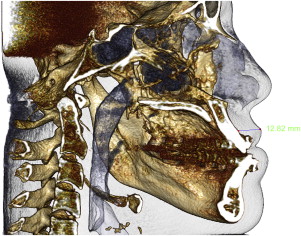
As presented in this article, a 3D model was created showing presurgical and postsurgical midface movement in relation to fixed bony structures. The presurgical and postsurgical CBCT volumes were imported into InVivo 5.1 (Anatomage, San Jose, CA). The 2 scans were superimposed onto a common Cartesian coordinate system using the skull bases as registration targets. The skull bases were outside the operative areas and expected to be morphometrically stable during the study period. The software used a voxel intensity minimization algorithm to register the 2 skull base volumes. The registered volumes could be viewed simultaneously and measured using digital calipers. This method allows for visualization and analysis of the hard and soft tissue changes. The analysis of a surgical patient was performed, with a primary focus on upper lip changes before and after Le Fort I osteotomy. Soft tissue measurements were taken from 3 points: subnasale, the most anterior lip projection ( Figs. 1 and 2 ), and stomion, on an arc taken from the odontoid process to the nasolabial fold. An example of a lip movement change at the vermilion border incorporating vertical change is shown after the patient’s Le Fort osteostomy ( Fig. 3 ), measured to be 7.84 mm.
Related posts:
 Foreword
Foreword
 3D and the Next Dimension for Facial Plastic Surgery
3D and the Next Dimension for Facial Plastic Surgery
 The Use of 3D Imaging Tools in Facial Plastic Surgery
3D Analysis of Tissue Expanders
The Use of 3D Imaging Tools in Facial Plastic Surgery
3D Analysis of Tissue Expanders
 Teaching 3D Sculpting to Facial Plastic Surgeons
Teaching 3D Sculpting to Facial Plastic Surgeons
 3D Volume Assessment Techniques and Computer-Aided Design and Manufacturing for Preoperative Fabrication of Implants in Head and Neck Reconstruction
3D Volume Assessment Techniques and Computer-Aided Design and Manufacturing for Preoperative Fabrication of Implants in Head and Neck Reconstruction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


