Fig. 1
Clinical photo from the lateral side of the leg demonstrating poor soft tissue envelope and anteromedial free flap. Note equinus position of the foot

Fig. 2
Clinical photo from the medial side of the leg with evidence of cellulitis

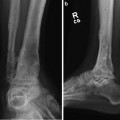
Fig. 3
AP radiograph demonstrating LDTA of 79° (86–92) representing valgus deformity and metaphyseal nonunion with intact hardware on the tibia and fibula

Fig. 4
Lateral radiograph demonstrating ADTA 85° (78–82) and a congruent articular reduction of the ankle joint. There is a very small segment of distal tibia

Fig. 5
Fifty-one inch standing erect leg radiograph demonstrating 23 mm limb length discrepancy, right short, and a mechanical axis deviation of 7 mm lateral
3 Preoperative Problem List
1.
Nonunion of a right type IIIB pilon fracture
2.
Post-traumatic bone loss , right ankle
3.
Suspected active infection
4.
Limb length discrepancy, right short, 2.3 cm
5.
15° right external rotation deformity
6.
15° right ankle equinus contracture
7.
Retained hardware right ankle
8.
Poor soft tissue envelope with wound dehiscence
9.
Small periarticular fragment and valgus deformity of the ankle
4 Treatment Strategy
This complex reconstruction was divided into two stages. We also discussed with the patient a salvage option, which would have been ankle arthrodesis. Stage one’s goals were to perform a meticulous ankle debridement and obtain reliable deep tissue cultures and pathologic specimens. A circular fixator would provide the stability. Dead space management after debridement would be managed with rapid shortening (2 mm per day) of the articular block to the distal metaphysis. The fixator would also correct the rotational and equinus deformity. Finally, residual limb length would be corrected with a proximal tibial and fibula osteotomy and application of TSF. Lengthening would be performed using the lengthening and then nailing (LATN) technique.
5 Basic Principles
Nonviable bone must be excised, potentially leaving a relatively small articular segment. If the tibial plafond is viable and good joint congruity exists, the ankle joint can be salvaged. 1.8 mm olive wires are used to secure the segment, and mechanical stability is augmented using a foot ring. The geometry of the bone resection is important. Flat cuts are mandatory. Soft tissue handling must be gentle, and a plastic surgery colleague is invaluable in choosing skin incisions as well as re-elevating soft tissue flaps. Spanning the ankle provides improved stability to the distal segment and can be used to correct ankle contracture or manage foot drop.
6 Images During Treatment
See Figs. 6, 7, 8, 9, 10, 11, 12, and 13
 8: Femoral Bone Defect
8: Femoral Bone Defect
 11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
 22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
 39: Ilizarov Ankle Fusion
39: Ilizarov Ankle Fusion
 63: Residual Clubfoot: Equinovarus Deformity/Knee Valgus/Limb Length Discrepancy
63: Residual Clubfoot: Equinovarus Deformity/Knee Valgus/Limb Length Discrepancy
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov




Related posts:
8: Femoral Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
39: Ilizarov Ankle Fusion
63: Residual Clubfoot: Equinovarus Deformity/Knee Valgus/Limb Length Discrepancy
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
