3 Mandibular Distraction
Introduction
Pierre Robin sequence (PRS), a triad of micrognathia, glossoptosis, and cleft palate, is the prototypical entity combining upper airway obstruction with cleft palate. Although Robin′s very first description of his eponymous sequence did not specifically include cleft palate, in all of his subsequent descriptions of PRS cleft palate is included as an integral feature.1–3 Furthermore, clinically significant upper airway obstruction from glossoptosis rarely occurs in nonsyndromic forms of micrognathia without cleft palate.4 It therefore seems proper and more clinically meaningful to define the triad of micrognathia, cleft palate, and glossoptosis as PRS. Other syndromic forms of PRS include mandibulofacial dysostosis (Treacher Collins syndrome), oculo-auricular-vertebral spectrum (Goldenhar syndrome), and Stickler syndrome. The clinical feature common to these infants is upper airway obstruction, specifically due to the intrusion of the base of tongue into the oropharynx (e.g., glossoptosis). Cleft palate may or may not be present and, in cases of Treacher Collins syndrome, choanal atresia may also affect airway patency.
Prenatal Evaluation
Modern obstetric management and high-quality fetal ultra-sound have identified infants with mandibular hypoplasia and the risk for upper airway obstruction at delivery.5,6 There is good evidence that the ex utero intrapartum treatment procedure is not indicated for the perinatal management of infants with severe, isolated micrognathia.7 How-ever, it is often prudent for the obstetrician to alert his/her pediatric otolaryngology colleagues. These mother–fetus cases can undergo multidisciplinary review to arrange for airway standby assistance at delivery, if necessary, for these high-risk deliveries.8
Initial Airway Evaluation and Management
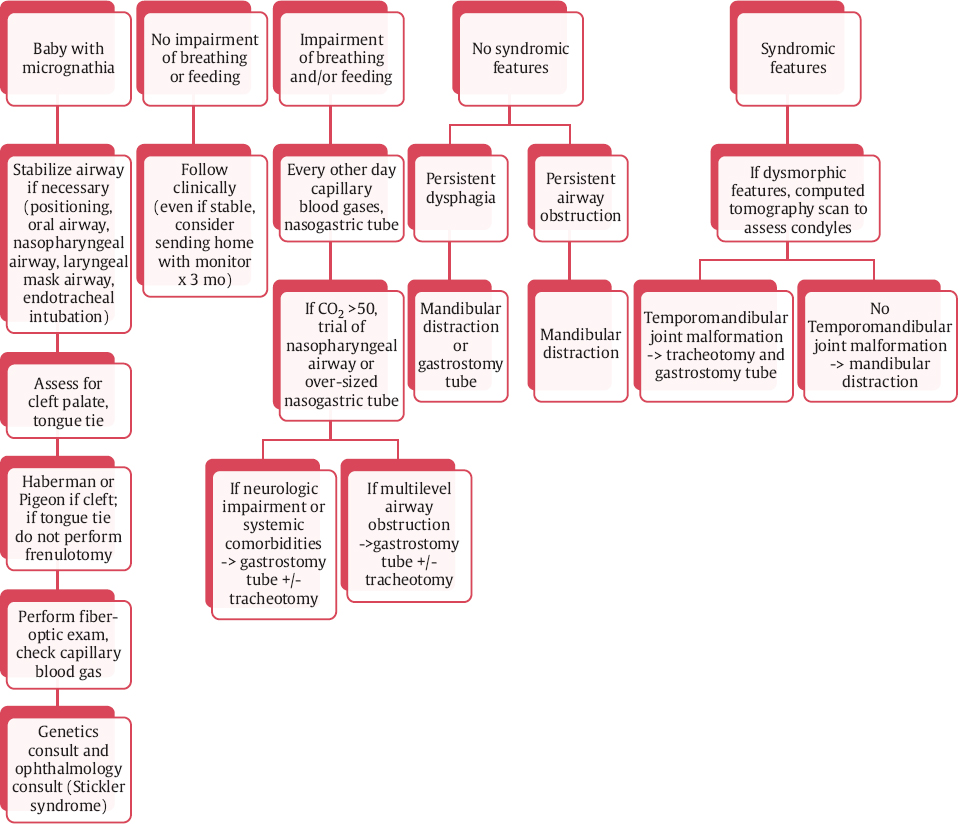
Newborns with glossoptosis present with varying degrees of upper airway obstruction. It often falls to the neonatologist and pediatric otolaryngologist to collaborate in the initial management of these infants ( Fig. 3.1 ). In the delivery room, the severity of airway obstruction ranges from minimal to life threatening. The clinical signs of significant airway obstruction include nasal flaring, substernal and/or intercostal retractions, sporadic or absent breath sounds on chest auscultation, poor oxygen saturations, cyanosis, bradycardia, and high pCO2 on initial blood gases.
It is easy for the clinician to underestimate the degree of upper airway obstruction based on simple observation. Newborns with significant upper airway obstruction may exhibit minimal oxygen desaturation and appear to be breathing normally; however, auscultation of the chest will often reveal only sporadic air movement. It often takes 30 to 60 seconds of careful auscultation to detect the gasps of breath that result in the sudden bursts of ventilation required to maintain near normal oxygen saturations. Use your stethoscope!
If a prenatally detected case of PRS is identified, the delivery room or neonatal resuscitation room should be equipped with a sterile set of infant tracheotomy instrumentation (although a minimal set of forceps, scissors, and scalpel will suffice in a true emergency), infant laryngoscope (Parsons 1 and 2), small endotracheal tubes (2.0–3.5 mm), small laryngeal mask airways, neonatal oral airways, and an ultrathin fiberoptic bronchoscope with a light source. Digital optical laryngoscopes are becoming increasingly available and can also be used when appropriate. A pediatric glidescope may be utilized; however, sometimes intubation with smaller endotracheal tubes using this device can be challenging, even if the view on the screen is adequate.
Although a stepwise approach to the establishment of an adequate airway is recommended, rapid progression through the following airway management algorithm is often required in children with micrognathia:
Position the infant on his/her side
Can be followed by prone positioning
If repositioning is unsuccessful, then place a nasopharyngeal airway/nasal trumpet
If unsuccessful, place an oral airway with bag-mask ventilation
A laryngeal mask airway (LMA) should be tried next (size 1 LMA)
Fiberoptic or glidescope intubation
Tracheotomy
Initial airway management should include side positioning followed by prone positioning. If repositioning is unsuccessful, the next option is placement of a nasopharyngeal airway (NPA), or nasal trumpet, being careful to ensure that the tip of the NPA extends beyond the base of tongue. The optimal position of the NPA can be confirmed by passing a flexible endoscope through the trumpet itself or through the contralateral nasal cavity.
For those newborns who are truly unable to ventilate, more invasive measures are warranted. The next set of interventions should begin with placement of an oral airway with bag-mask ventilation. If an oral airway cannot be inserted, an LMA should be tried next. The size 1 LMA can be a life-saving device in newborns with PRS. In a recent case series of 123 newborns with micrognathia encountered at two institutions over a 10-year period, all were able to be managed with an LMA as a bridge to intubation or tracheotomy.7 Pediatric intubating LMA devices may also be utilized successfully. However, rarely micrognathia is associated with significant ankylosis of the mandible (arthrogryposis multiplex congenita), and limited jaw opening may not allow for insertion of an LMA. When LMA placement is unsuccessful or adequate ventilation still not possible, then a quick attempt at transoral endotracheal intubation should be made using a small straight laryngo-scope or digital optical laryngoscope (Parsons 1 or 2, pediatric glidescope). However, in most cases when the previous strategies have failed, transoral intubation is unlikely to succeed and therefore minimal time should be wasted before subsequently attempting flexible transnasal fiber-optic intubation. Success with this approach often depends on the experience of the endoscopist and the ability of the infant to maintain some degree of ventilation with spontaneous effort. The absence of a nasal floor due to the cleft palate may be quite disorienting if not anticipated. Utilizing an assistant to pull the tongue forward by grasping the anterior tongue with a penetrating towel clamp, small Allis clamp, or a tongue stitch is also extremely useful and is often the difference between a successful fiberoptic intubation and disaster. Simultaneous insufflation of oxygen via transnasal placement of an endotracheal tube or nasal trumpet through the contralateral nostril may facilitate successful transnasal fiberoptic intubation.9
If transnasal intubation fails, emergent tracheotomy should be performed. In contrast to the emergent adult airway, cricothyroidotomy is not a recommended approach for the establishment of the emergent pediatric airway due to the risk of severe iatrogenic glottic and subglottic stenosis. Cricothyroidotomy also offers no distinct advantages over expeditious formal infant tracheotomy—a procedure that, in most experienced hands, can be performed within a minute or two.
Relationship Between Airway and Feeding
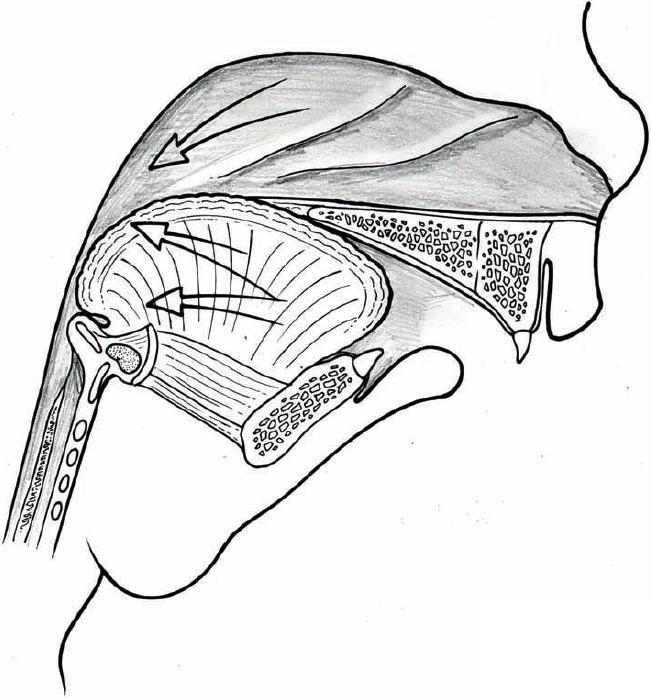
An overarching theme in the management of the glossoptotic infant is the causal relationship between airway obstruction and feeding efficiency. An infant with normal oropharyngeal anatomy is able to breathe and feed simultaneously (a feat that results in choking, gasping, and aspiration if attempted in older individuals). This ability is related to at least two characteristics of the infantile larynx, including (1) a cephalad position of the infantile larynx compared to an adult, and (2) its interdigitation with the uvula and soft palate. This relationship produces an effective separation of the air exchange occurring between the nasal cavity, larynx, and tracheobronchial tree anteriorly within the laryngopharynx and the upper digestive tract of the oral cavity, oropharynx, hypopharynx, and esophagus posteriorly and laterally.
Within the first few months of life, growth in the dimensions of the head and neck and the relative descent of the larynx results in the loss of this ability to breathe and feed simultaneously. However, this sequence occurs after the infant has developed sufficient oral motor coordination to maintain effective deglutition and swallowing without aspiration. Clinical experience would suggest that this degree of coordination is not present at birth. Infants who lack a normal relationship between the tongue, soft palate, and larynx will suffer varying degrees of feeding difficulties.
Infants born with abnormalities affecting the tongue, soft palate, and larynx frequently suffer with feeding difficulties and are at risk for failure to thrive. It also follows that more severe abnormalities can result in greater feeding difficulty. The feeding difficulties observed in nonsyndromic infants with glossoptosis are best explained by the abnormal anatomic relationships between the tongue, palate, and larynx rather than an intrinsic feeding abnormality or neuromuscular disorder. Failure to thrive is consequent to (not merely coincident to) the airway obstruction in infants who are neurologically normal.
Assessing the Need for Further Intervention
As the degree of airway obstruction in the glossoptotic infant is widely variable, so is the need for further airway intervention after birth. Infants with minimal or no detectable airway compromise often require little more than assessment of their feeding abilities and monitoring of weight gain during the first few months of life. At the other extreme are the infants who require establishment of an artificial airway (e.g., LMA, endotracheal tube, or tracheotomy) during the first few hours or days of life. These infants are at greater risk to require a definitive surgical intervention to establish an adequate airway.4 Between these two extremes is a vast middle spectrum of airway and feeding compromise, and treatment is based on clinical judgment and experience.
Airway Obstruction
There are a variety of options available for airway management in the micrognathic child. The management of acute airway obstruction in newborns with PRS was described earlier. The approach to managing more indolent, chronic airway obstruction in neonates is different. When an otherwise stable newborn displays signs of chronic upper airway obstruction, it is most reasonable to begin with conservative measures first. Prior to intervention, the airway should be assessed with bedside flexible laryngoscopy to rule out a synchronous airway lesion. These can include choanal atresia (sometimes seen in Treacher Collins syndrome), laryngomalacia, or a glottic web with or without subglottic stenosis (velocardiofacial syndrome). The presence of an additional site of airway obstruction may suggest the need for intervention and may influence the choice of definitive surgical airway intervention. In instances of significant multilevel obstruction, it is most prudent to move forward with tracheotomy to definitively secure the airway until these sites of obstruction can be addressed sequentially.
In the most common scenario of mild to moderate or intermittent obstruction (episodic oxygen desaturations at rest or with feeds, signs of chronic respiratory acidosis on capillary blood gas, inability to ingest an adequate volume of oral feeds), the authors’ philosophy is to start with side and prone positioning. If this fails to improve ventilation, placement of a nasopharyngeal airway or nasal trumpet to bypass tongue base obstruction and break the seal made between the oropharyngeal tongue and the posterior pharyngeal wall may prove more effective. A variety of custom oral appliances may be fashioned for the purpose of relieving obstruction.10–12 Other authors have described success at simply customizing a nasoendotracheal tube to relieve obstruction.13 Nonsurgical management of upper airway obstruction in children with PRS is always preferable. Most case series examining airway interventions in infants with PRS demonstrate that over half of these children may be successfully managed nonoperatively.4,14–19 The decision to move forward with a surgical intervention remains controversial. A decision should be made based on objective evidence, including trends in pulse oximetry, carbon dioxide levels, feeding trends, and polysomnography if warranted. The authors’ threshold for surgical intervention and the preferred methods of intervention for airway and feeding difficulty in neonates with PRS are discussed later in this chapter.
Feeding Difficulty
A fairly consistent feature of infants with PRS is the inconsistency of airway obstruction and feeding difficulty. It is almost axiomatic that these infants will have good days and bad days with respect to their feeding performance and breathing difficulties. The clinical challenge is to determine the overarching trend of these difficulties. Many infants with PRS may demonstrate occasional daily success in feeding; however, over the first few weeks of life, they will fail to maintain adequate weight gain. In contrast, some infants will demonstrate periodic difficulties with feeding and weight gain, but the overall trend demonstrates adequate feeding and weight gain. The lesson from years of observing hundreds of infant with PRS is clear: in most cases, a period of 7 to 14 days of hospitalized observation is required to determine the feeding trend of any individual infant.
Feeding Guidelines, Strategies, and Assessment
The feeding performance of an infant with PRS is observed for 7 to 14 days. A number of objective criteria are available to aid in the assessment of the need for additional intervention. At our respective institutions, we primarily rely on feeding trends, obstructive events, carbon dioxide retention, and weight gain. We would expect a formula-fed/-supplemented child with a cleft palate to regain his or her birth weight by 2 weeks of age. Serial capillary blood gases (drawn in the morning and not after a prolonged period of stimulation, crying, or activity) should demonstrate pCO2 levels in the 40s. When levels increase into the 50s and the bicarbonate level rises (suggesting metabolic compensation of a chronic respiratory acidosis), a higher suspicion for chronic airway obstruction should exist. If the child is clinically faring poorly, these more objective measures may offer support for an intervention. Polysomnography may also be performed; however, we tend to rely on these other objective measures in the neonatal period, as neonatal polysomnography is difficult to interpret and not always reliable.
Feeding Trends
The infant with PRS must overcome the inherent difficulty of feeding with a cleft palate as well as the added burden of a variable degree of airway obstruction from glossoptosis. General feeding strategies begin with the same principles of any child with cleft palate: the absolute admonition to avoid attempts at direct breast-feeding, recommendations for pumping mother′s breast milk for delivery by bottle, and the use of a special bottle/nipple to facilitate delivery of breast milk or formula without the need for an effective suckle (e.g., Haberman feeder, Mead Johnson cleft palate nurser, pigeon nipple; see Chapter 1).
Failure to thrive in the PRS population is due to two mechanisms that are not mutually exclusive: caloric intake and work of breathing. Consultation with an experienced feeding therapist (occupational or speech therapist, or feeding nurse specialist) should be initiated for any newborn noted to be struggling with feeding. In some cases, members of the neonatal feeding team can successfully feed such infants, but may find that the rest of the nursing team has variable results. In these cases, the family is rarely able to achieve similar feeding volumes as well. Common problems are failure to achieve adequate caloric intake despite supplementation with high calorie formula or prolonged feeding times leading to progressive fatigue and decreasing feeding efficiency. Sometimes, feeding difficulties are ameliorated with placement of a nasopharyngeal airway owing to relief of airway obstruction. Other times, feeding is negatively impacted by the presence of an airway device, and these need to be removed during feeds. In the long run, failure to translate successful feeding strategies to the infant′s direct caregivers will result in failure to thrive and thus necessitate surgical intervention. The need for direct professional-to-family education in feeding technique cannot be overstated.
Even in cases in which adequate caloric intake is achieved, the infant may still demonstrate failure to thrive. In such cases, it becomes important to reassess the work of breathing to overcome upper airway obstruction. This effort results in an increased caloric expenditure, which contributes to failure to thrive. While this situation may be temporarily addressed with fortification of the breast milk or formula, this strategy merely addresses one symptom of the underlying problem—significant upper airway obstruction—and is usually not a sustainable “solution” as the child grows.
Again, it must be stressed that poor feeding performance in PRS is primarily due to the airway obstruction, and inherent feeding disorders are less commonly the problem.
Feeding Tubes
Infants who are struggling to develop successful oral feeding performance will often benefit from supplementation via orogastric or nasogastric feeding tubes. A number of strategies may be used to manage these supplemental feedings with the overarching goal of providing adequate nutrition without adversely affecting the infant′s ability and desire to feed orally. It is advisable to maintain a normal oral feeding schedule with attempts at oral feeding at regular intervals. Any deficiencies of the desired oral intake volume can be delivered via gavage feed. The time allowed for oral feeding should be limited to prevent the infant from becoming fatigued and frustrated. A typical plan might call for 60 mL every 3 to 4 hours with limiting oral feeding time to no more than 20 to 30 minutes. If the infant successfully takes the full volume in the allowed time, then no gavage is required. However, if only 20 mL is taken orally, an additional 40 mL is delivered via naso-gastric tube at the conclusion of the feeding session. This sequence is repeated, adjusting the gavage volumes with each feeding accordingly.
This strategy provides for adequate caloric intake regardless of oral feeding performance, keeps the infant on a regular feeding schedule, and avoids persistent satiety. Compliance with such a programmatic feeding strategy also provides adequate data to assess the feeding trend and allows the clinician to make an objective declaration regarding success or failure to thrive. Asking the nursing team to construct a histogram displaying daily intake over several days allows for a graphic representation of oral and supplemental intake and may be extremely helpful in communication between families and providers alike. We have also observed that premature abandoning of oral feeding and placement of a feeding gastrostomy is seen to occur in institutions that lack experience with feeding infants with PRS. An infant with poor feeding but a passable airway is thereby given a feeding gastrostomy, which can lead to the development of prolonged oral aversion.
Inpatient versus Outpatient Management
If the infant does not demonstrate consistent upper airway obstruction as determined by oxygen desaturations, apneic spells, and pCO2 levels, and achieves adequate initial feeding performance, outpatient management may be considered if the airway has been stabilized with positioning or use of a nasal trumpet alone. In these cases, one must establish a reliable and effective outpatient monitoring strategy. It is important to understand that a significant subset of these early achievers will suffer increasing airway obstruction with deterioration in feeding performance within the first 2 to 6 weeks of life. If the physician feels that community resources are inadequate or the family is unreliable, continued inpatient observation with transfer to a special care nursery or similar setting should be continued for at least the first 4 to 6 weeks of life or until a satisfactory outpatient monitoring program can be established in order to assure regular weight gain.
Weight Gain
Weight gain remains the single most important objective indication of feeding performance. We apply the same weight gain criteria in PRS as any child with cleft palate. As with most infants, those with PRS will experience weight loss during the first week of life. However, the infant should return to his/her birth weight by 14 days of age and subsequently demonstrate a minimum weight gain of 4 ounces (~115 g) per week thereafter. Outpatient infants should be weighed weekly on the same scale either at the primary care physician′s office or at home by a visiting nurse. For outpatients, failure to achieve weight gain goals for more than 3 weeks in a row should result in hospitalization to begin reassessment of feeding performance and airway obstruction.
Surgical Interventions
Supportive Airway Interventions
Although many children with PRS may be stabilized with positioning or use of an oral appliance, some patients are unable to tolerate oropharyngeal stents or nasopharyngeal airways, as management of these devices may prove overwhelming to providers and parents alike. For those children that have success with airway appliances, newborns may be discharged home with the device in place, with close outpatient monitoring of the feeding metrics described above. Airways are maintained for weeks to months, with a gradual plan of transitioning to use of the device only at night prior to ultimate discontinuation. For those infants with PRS who ultimately fail noninvasive management strategies, a variety of surgical interventions for addressing tongue base obstruction exist. Multiple glossopexy procedures have been described. Tongue-lip adhesion (TLA) can performed with or without subperiosteal release of the floor of mouth and circummandibular suturing.20 One widely practiced technique involves release of genioglossus musculature from the mandible followed by circummandibular suturing of the tongue base to the mandibular symphysis. Mucosal flaps raised from the ventral tongue and gingivolabial sulcus are approximated to complete the adhesion.21 The adhesion may be maintained throughout the first year of life, and subsequently taken down at the time of cleft palate repair.
Although the success of this technique at managing airway obstruction may be as high as 89% in select patients,21 tethering the mobile tongue anteriorly will exacerbate the child′s underlying dysphagia, assuring a prolonged period of enteral feeding supplementation via nasogastric catheter or gastrostomy tube.15,16,21 In 1998, a survey of airway surgeons at pediatric centers caring for children with PRS suggested that over 80% of institutions have abandoned this technique22; however, the minority of centers who still employ TLA believe it is a worthwhile intervention and are satisfied with their results.16,21 Advocates cite the relative simplicity of the procedure, lack of long-term scarring, avoidance of potential nerve or tooth injury, and lack of specialized equipment as major advantages of the TLA technique over more complex and expensive orthognathic procedures. Critics of the technique cite variable results and significant postoperative dysphagia requiring prolonged nasogastric or gastrostomy tube feeding. Additionally, the circummandibular stitch causes an iatrogenic cleft in the inferior alveolus, splaying the inferior central incisors. It is the authors’ opinion that those children who can be stabilized with TLA are likely the same group of patients who may be successfully managed with nasopharyngeal airways with or without nasogastric feeding. For this reason we do not routinely perform this intervention, offering TLA to only those families who decline mandibular distraction osteogenesis but wish to attempt an alternative intervention prior to moving forward with a definitive tracheotomy.
Traditional algorithms for airway management in children with PRS point to the use of tracheotomy as a final backup for children that fail TLA, as tracheotomy is a definitive technique for securing a stable airway in any patient with upper airway obstruction. Although a tracheotomy will reliably and successfully bypass the site of tongue base obstruction, it is a procedure with potential long-term morbidity and mortality.23,24 Complications associated with tracheotomy include sudden airway obstruction from accidental decannulation or mucous plugging as well as airway infections, bleeding, stomal maintenance problems, tracheal stenosis, and inhibition of proper speech and swallowing development. Furthermore, children with tracheotomies require skilled nursing care at home and in their educational facilities, along with monitoring and suction equipment among other resources. Nevertheless, in a survey of otolaryngologists at large fellowship training centers, 52% chose tracheotomy as the treatment of choice for airway management in children with PRS.22
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


