3. Analysis of the Neck
3.1 Introduction
Proper assessment is the first step and one of the most important steps in the planning of any plastic surgery procedure. The desired cosmetic outcome can be achieved only if a proper history is taken and a physical examination is performed before undertaking any treatment. Lack of understanding and appreciation of the issues faced is a frequent cause of complications and undesirable results. 1
3.2 Patient’s Concerns
The first step is always to inquire about the patient’s concerns, needs, and desires. The neck can relay an image of youth, fitness, strength, and vitality or one of age, obesity, weakness, or illness. These perceptions affect how we see ourselves and how we view others. It is important to explore the patient’s motivation for seeking surgery, as well as the anticipated cosmetic and emotional outcomes. The patient’s concerns should be the priority, and these concerns must be specifically addressed. The surgeon should discuss additional related problems and explain their relevance to the patient. Educating the patient and allowing him or her to participate in the process is empowering and allows the treatment plan to suit the patient’s needs. This approach is most likely to lead to the best outcome for that individual patient.
Evaluating photographs of the patient at a younger age may help reveal relevant anatomy camouflaged by the signs of aging and can also serve as a goal for the anticipated rejuvenation procedure. Photographs of others whose features are considered desirable by the patient can also serve as a great communication tool, giving the surgeon better insight into the patient’s sense of aesthetics and expectations from the contemplated procedure.
3.3 Medical History
A thorough medical history should be taken, including the patient’s general health and an assessment of anesthetic risk. A history of risk factors for intraoperative bleeding, as well as difficulties healing after any surgical procedure, may influence the treatment choice significantly. History of hypertrophic scars or keloids should be noted. Smoking may lead to major healing problems, especially in a neck lift, and accurate history should be emphasized to the patient.
Prior surgical cosmetic procedures to the face and neck, such as mandibular surgery, chin augmentation, submental liposuction, plication of the platysma, or neck lift, may influence the procedure choice and technique. A history of head and neck tumors, radiation, or skin cancers is also of great importance and should not be overlooked.
3.4 Congenital Disorders of the Skin
The surgeon needs to be aware of certain rare congenital disorders of the skin. Cutis hyperelastica (Ehlers-Danlos syndrome) is characterized by very thin, friable skin that can be stretched an inordinate amount but retracts to normal thereafter. Hypermobile joints and subcutaneous hemorrhages may be seen in patients with this disorder. Because of the high risk for poor wound healing, as well as bleeding, most procedures of the neck are to be avoided. In cutis laxa, the skin lacks elasticity and does not recoil; however, it heals normally. Rhytidectomy can be rather beneficial to these patients, without a significant risk. Pseudoxanthoma elasticum is quite similar to cutis laxa and is differentiated by skin biopsy; rhytidectomy is also frequently beneficial for patients with this condition. Progeria (Hutchinson-Gilford syndrome) patients have multiple severe problems and a short life expectancy; therefore, plastic surgery is not a consideration. Adult progeria (Werner’s syndrome) is extremely rare and is characterized by scleroderma-like scattered patches, baldness, skin pigment irregularities, and facial aging. Patients may have short stature, a high-pitched voice, cataracts, muscle atrophy, atherosclerosis, diabetes mellitus, and various tumors. Elective surgery is not recommended.
3.5 Aesthetic Evaluation of the Neck
The first impression of examination should always be remembered and should be an important factor in developing a treatment plan. The features that distort the harmony of the face and neck and stand out should always receive the most attention. Balance and harmony of the face and neck must be a priority over minor imperfections. Whatever distracts and is noticed by the surgeon before the detailed evaluation is likely to evoke the same response in most other people.
The neck should never be evaluated in isolation; rather, its relationship to the shoulders, and especially to the face, needs to be considered. It is crucial to maintain, or create if necessary, appropriate proportions between the neck and the face. They are seen together and influence each other’s appearance tremendously. The level of rejuvenation planned for the face and the neck should also match, and they should look like they belong together and to the same body.
3.5.1 What Is a Youthful Neck?
Before looking at the specific features and details during examination, it is important to define what is generally considered a youthful and attractive neck. These features were well described by Ellenbogen and Karlin (Fig. 3.1): 2
Well-defined inferior mandibular border
Subhyoid depression
Visible thyroid cartilage
Visible anterior border of the sternocleidomastoid muscle
Cervicomental angle of 105 to 120 degrees, submental–sternocleidomastoid (SM-SCM) angle of 90 degrees
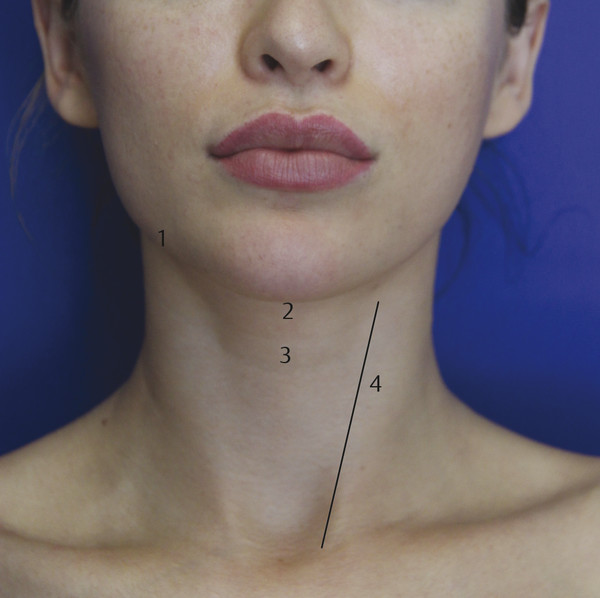
Fig. 3.1 Landmarks of a youthful neck. (1) Well-defined inferior mandibular border, (2) subhyoid depression, (3) visible thyroid cartilage, and (4) visible anterior border of the sternocleidomastoid muscle.
Inferior Mandibular Border
Starting the examination with the bony structure is helpful. The size of the mandible, its width, and the chin projection play a large role in giving a well-defined inferior mandibular border. Achieving the perfect contour may be challenging. Any excess of subcutaneous fat would obscure the inferior mandibular border in a patient with even relatively mild micrognathia or retrognathia. Jowling would also show an additional contour irregularity. Neck surgery alone might not be sufficient to achieve a clean inferior mandibular border, especially if significant jowling is present. Evaluating the face and planning a concurrent facelift should be considered.
Hyoid Bone Position
The position of the hyoid bone is extremely important in allowing an optimal cervicomental angle to be achieved. 3 , 4 Like the mandibular shape, the hyoid position is a gift or a challenge that we receive at birth. When the hyoid is positioned low, the result is a blunt cervicomental angle that is greater than 120 degrees. It frequently gives the appearance of excessive submental fat and lack of definition. In a fatty neck, the hyoid may be difficult to palpate. It is helpful to know its position preoperatively, thus enabling better surgical planning and a more accurate gauge of the likely postoperative outcome. (Fig. 3.2 and Fig. 3.3).

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


