25. Management of the Lateral Periorbital Area
25.1 Introduction
Dr. Connell has always emphasized maintaining facial harmony during any facial rejuvenation surgery and avoiding complications. He stressed the importance of the surgeon’s ability to look at an aging face as a whole and form a vision of what would look good and what procedure or procedures would be appropriate for that patient. Management of the aging face is really to maintain a patient’s appearance, not to change it. Look at old patient photos for guidance. The goal is not only to look your best at your current age, but also to look age appropriate.
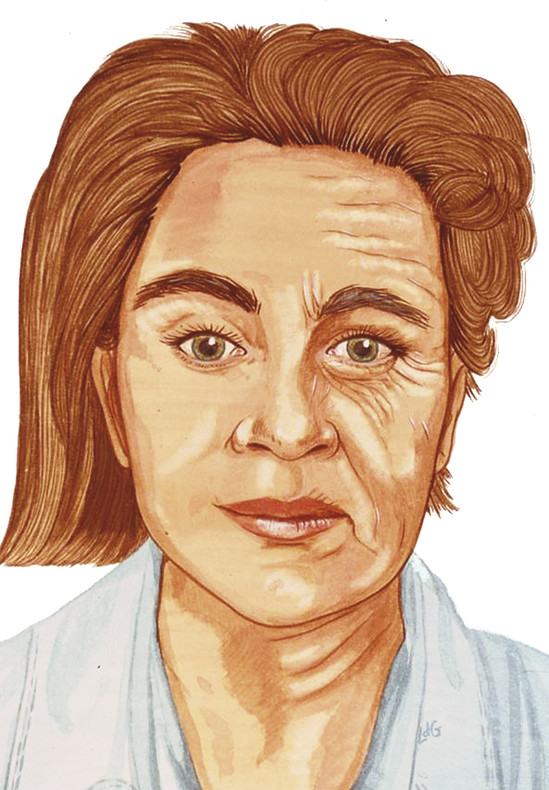
As the face ages, there are many signs that are consistent. The lateral periorbital area shows some of the earliest signs of the aging process. Two consistent signs of the aging process are lateral periorbital rhytids (crow’s feet) and a degree of ptosis of the lateral brow. These early signs of the aging process often become apparent in the third and fourth decade of life (Fig. 25.1).
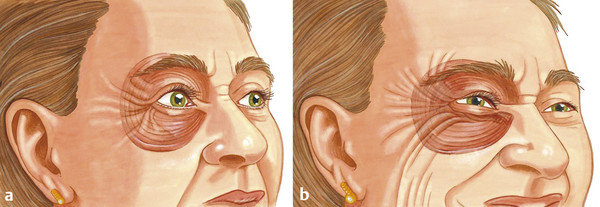
The orbicularis oculi muscle is the unopposed depressor of the lateral brow. The sphincter action of the orbicularis oculi muscle is responsible for creating rhytids in aging skin, especially in the lateral periorbital area (Fig. 25.2). In many aging faces, ptosis may occur over the entire brow and may result in the individual compensating by elevating the brows with frontalis muscle action.
25.2 Compensated Brow Ptosis
When the frontalis is activated, typically, the medial and central brows are elevated, but not the lateral brow; there is no elevator of the lateral brow. Compensated brow ptosis results in an aging pattern of the forehead with horizontal skin creases from frontalis muscle contraction and ptosis of the lateral brow that is typically more evident than that of the rest of the brow.
If the overall brow is ptotic, a full browlift may be indicated. If only the lateral brow is ptotic or if the patient refuses a full browlift, however, a form of a lateral browlift may be indicated. In my opinion, many patients who are in their 40s and 50s, and older might not need a full browlift as part of their facial rejuvenation. If that is the case, then an isolated temporal browlift or an extended temporal incision during facelift surgery will allow access to subcutaneous undermining of the lateral periorbital area. Even with a full browlift, an extended temporal incision during a concurrent facelift and neck lift surgery will redrape the skin overlying the lateral orbicularis oculi muscle.
This redraping will “reset” the skin contraction pattern of the overlying periorbital skin with the underlying orbicularis oculi muscle. This skin “reset” is the key to long-term improvement in the appearance of lateral periorbital rhytids. Redraping alone will improve the appearance of crow’s feet for a prolonged period. Also, redraping the temporal skin flap superiorly elevates the lateral brow.
25.3 Lateral Periorbital Aging
The following are the three Ds of the facial aging process specific to the lateral periorbital area:
Deflation: Loss of fullness in the temporal hollow.
Descent: Lateral brow ptosis due to both orbicularis oculi muscle action and gravitational pull.
Deterioration: Overlying skin creasing due to loss of collagen and elastin seen with the aging process; this is even more evident in the periorbital area owing to the very thin dermis.
The orientation of the lateral periorbital skin over the underlying orbicularis oculi muscle fibers has been consistent as the patient ages. The development of radial creasing in the lateral periorbital region is a result of the sphincter action of the underlying orbicularis oculi muscle. With time, the ability of the overlying skin to contract on itself with the underlying sphincter muscle contraction fades. Rather than the skin contracting on itself, as in our younger years, it is increasingly thrown into folds. The skin creasing and folding pattern becomes etched into the skin over time. This consistent pattern of underlying muscle contraction and overlying skin creasing and folding results in a recurrent specific pattern of crow’s feet. Although the use of a neuromodulator to reduce the underlying muscle contraction and a “skin treatment” to attempt to improve skin quality may be helpful, it is the “reorientation” of the overlying skin on the underlying muscle that is the key to long-term improvement in the appearance of lateral periorbital rhytids. By undermining the skin in the subcutaneous plane and redraping the skin in a superior and slightly posterior direction, the “new” orientation of the preexisting cutaneous rhytids to the underlying muscle will reestablish how the skin will contract.
Related posts:
 6. Facial Sculpting and Facial Slimming with Neurotoxins
6. Facial Sculpting and Facial Slimming with Neurotoxins
 20. Comparison of Midface Rejuvenation Techniques
20. Comparison of Midface Rejuvenation Techniques
 22. Lower Eyelid Blepharoplasty
22. Lower Eyelid Blepharoplasty
 5. Energy-Based Treatments for Facial Aging
5. Energy-Based Treatments for Facial Aging
 9. Male versus Female Facelift Surgery. Is There a Difference?
9. Male versus Female Facelift Surgery. Is There a Difference?
 12. Primary Superficial Musculoaponeurotic System (SMAS) Facelift and Neck Lift
12. Primary Superficial Musculoaponeurotic System (SMAS) Facelift and Neck Lift
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


