Fig. 1
Clinical photograph of the patient after damage control external fixator has been placed. The patient had severe crush injury to the distal leg with nonviable skin and muscle
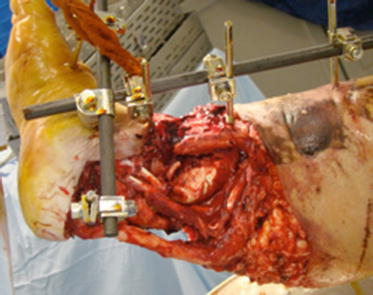
Fig. 2
Clinical photograph of the patient post-debridement. Extensive debridement was necessary to remove any nidus for future infection that would compromise limb viability
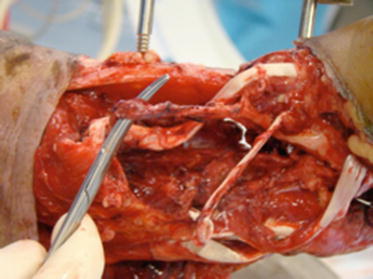
Fig. 3
Intra-operative photograph after identification of at-risk structures (neurovascular bundle)
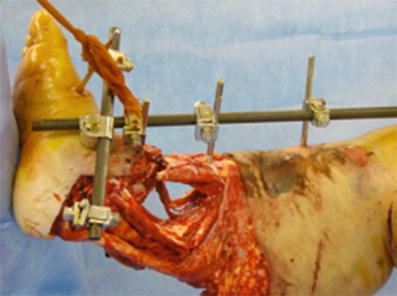
Fig. 4
Damage control external fixator maintained for limb stability during initial reconstructive efforts

Fig. 5
Clinical photograph of the patient’s limb post-debridement. Note the circumferential skin, subcutaneous tissue, muscle, and bone loss
3 Preoperative Problem List
1.
Severe trauma to the leg with circumferential skin, muscle, and bone loss
2.
s/p type IIIC distal tibia fracture
3.
Exposed neurovascular structures
4.
Distal tibial bone loss
5.
Loss of ankle joint
4 Treatment Strategy
Aggressive damage control orthopedics. This involves limb stability with “trauma” external fixator, serial debridements, early soft tissue coverage, and dead space management.
Acute shortening technique to decrease the bone and soft tissue defect.
“Orthoplastic” approach. Early involvement with a plastic and reconstructive surgeon experienced in limb salvage is critical.
Soft tissues stability and multiple muscular flaps.
5 Basic Principles
Immediate antibiotic therapy
Stabilization of bone and soft tissues at index surgery
Staged use of circular external fixation , especially if free flaps are necessary (limits surgical exposure for plastic surgeons)
Early bone coverage with muscular flaps
6 Images During Treatment
See Figs. 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, and 18.



 8: Femoral Bone Defect
8: Femoral Bone Defect
 11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
 22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
 39: Ilizarov Ankle Fusion
39: Ilizarov Ankle Fusion
 63: Residual Clubfoot: Equinovarus Deformity/Knee Valgus/Limb Length Discrepancy
63: Residual Clubfoot: Equinovarus Deformity/Knee Valgus/Limb Length Discrepancy
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov




Fig. 6
Acute shortening and segmental bone stability
Fig. 7
Muscular rotational soleus and gastrocnemius flaps
Related posts:
8: Femoral Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
39: Ilizarov Ankle Fusion
63: Residual Clubfoot: Equinovarus Deformity/Knee Valgus/Limb Length Discrepancy
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
