23 Endoscopic Repair for Septal Perforation: Algorithm
23.1 Introduction
Nasal septal perforation (NSP) repair remains a challenging issue for rhinologists—not only due to its technical aspects but also in choosing the most suitable approach concerning the specific nasal anatomic situation in addition to the surgeon’s experience.
The goal should be to provide a closure for the NSP without tension, restore the normal intranasal function, and, in some cases, to reconstruct the nasal support.
NSPs are usually an incidental finding in asymptomatic patients during physical examination. If there are no complaints, no treatment is necessary, and when the perforation causes only mild symptoms, conservative management can be attempted at first, such as nasal irrigation with isotonic saline and/or antibiotic ointment.
If complaints persist despite nonsurgical therapy, surgery should then be considered. Although many surgical techniques for the repair of NSP have been attempted for many decades, no agreement has yet been reached on the most suitable method for the best outcome.
NSP can be repaired with different approaches, such as external rhinoplasty, intranasal (endoscopic or microscopic), sublabial, and midfacial degloving. 1
A literature review published in 2007 did not make any significant conclusion regarding the relative rate of success for the various techniques used to close NSP. 1
Over the last decade, a wide variety of endoscopic endonasal approaches (EEAs) have been described for the treatment of NSP. Case series and case reports showing favorable outcomes via an EEA have recently increased despite its technical difficulties, particularly in cases of small to moderate perforations by the benefit of the endoscopic technique. 2 , 3 , 4 , 5 , 6 , 7 , 8 , 9 , 10 , 11 , 12 , 13 , 14 , 15
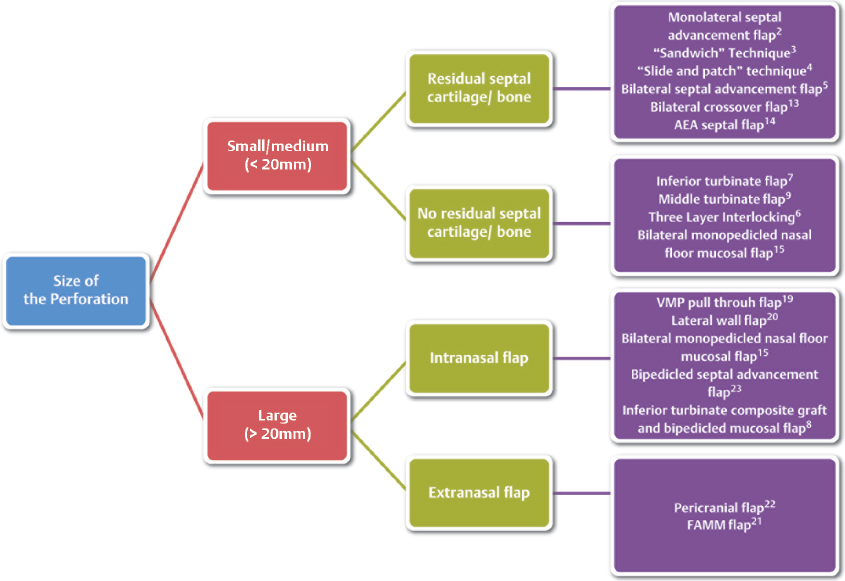
Depending on the size of the perforation and nasal anatomic condition, treatment method and flap choice may differ. This chapter provides a decisional algorithm on different endoscopic techniques regarding several local aspects (e.g., size and location of the defect, previous septal surgery).
23.2 Relevant Analytical Factors
NSPs located in the posterior part of the septum tend to be asymptomatic, whereas anterior perforations often present symptoms (e.g., crusting, a sensation of nasal obstruction, bleeding, headache, dryness, and whistling); thus we considered only the latter as candidates for surgery.
Measuring the size of the perforation preoperatively is an important factor for planning the operation; however, the size usually increases with elevation of mucoperichondrial flap and trimming margins.
According to current literature, NSP may be stratified based on size as follows: small perforations 0.5 cm or less, medium perforations between 0.5 and 2 cm, large perforations greater than 2 cm.
Although defects larger than 2 cm in length are generally accepted as a large size, the upper limit of small size differs between authors, up to 0.5 or 1 cm. 16 , 17
Computed tomographic (CT) scan of the paranasal sinus is an evaluation tool used not only to measure the septum defect but also to evaluate the amount of residual bone/cartilage.
In NSPs that have occurred after septoplasty, there is usually very little cartilage left, and this makes dissection of the flaps more difficult.
For small- to middle-sized NSP, different techniques require a nasal septum with a residual underlying cartilage or bone, which help perform a meticulous dissection to elevate the mucoperichondrium-mucoperiostium. 2 , 3 , 4 , 5 , 13 , 14
For these types of techniques, which use mucoperichondrial and mucoperiosteal septal tissue to close the perforation, the amount of septal structures remains as fundamental prognostic indicator of successful surgery.
Therefore, when it is not possible to perform an easy dissection of the septal mucosa, it is preferable to choose alternative techniques that use mucosal flaps harvested in other anatomical areas. 6 , 7 , 8 , 9
It is also important to check the quality of the intranasal anatomical structures preoperatively, which represented potential donor sites of grafts or flaps (inferior turbinate, middle turbinate, floor of the nasal fossa). Several local or regional flaps have been described for closure of septal perforations, but in our opinion, only the techniques adopting nasal mucosal flaps achieve normal nasal physiology because they use the normal respiratory epithelium for closure.
Small to moderate perforations can be repaired with local advancement flaps alone or combined with interposition grafts. Some centers have reported good outcome without interposition grafts, and the promising results show that the need for an interposition graft has not been established yet. 13 , 14 , 15 , 18
Nevertheless, according to different case series outcomes, in small and medium perforations (< 2 cm), the interposition of a graft between the two mucosal layers is, in our opinion, useless.
A recent systematic review found that interposition grafts appeared to help closure, as a template for mucosal migration during the healing process, but this factor was not considered statistically significant. 16 About the necessity for bilateral flap provision, unilateral flap coverage was advocated by some authors, as it limits the donor area to one side of the nose, and thus preserves more nasal respiratory mucosa while achieving favorable closure rates. 2 , 3 , 4 , 5 , 6 , 7 , 8 , 9 , 10 , 11 , 12 , 13 , 14 Even in patients with moderate to large perforation, complete closure can be obtained by applying a unilateral well-vascularized mucoperiosteal flap. 19
Large perforations with previous history of extensive septal trauma or surgery, however, cartilaginous remnants are usually insufficient and their quality can be quite low. In this situation, it is better to use mucosal flaps harvested in other anatomic sites (lateral nasal wall flap, facial artery musculomucosal flap, pericranial flap) 20 , 21 , 22 and adopt autologous graft materials to reconstruct the nasal support; for example, conchal cartilage is a good option if septal cartilage is not available. 6 , 23
We propose this algorithm for the endoscopic endonasal techniques for NSP repair (Fig. 23‑1).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


