23 Breast Surgery in the Male Patient
Abstract
Ideal surgical correction should be single staged, reproducible, minimize scars, and produce acceptable results with few complications. Male breast deformities in postbariatric and gynecomastia patients with severe deformities usually do not have satisfactory outcomes with limited-incision or minimally invasive procedures. The technique described here has evolved to preserve the nipple–areola on a thin inferior pedicle with reliable circulation, sensitivity, and satisfactory contour. The disadvantages seen in other procedures, including contour irregularities, nipple–areola depigmentation, and loss of sensitivity, have been avoided. The single long scar, although placed in a satisfactory anatomic position, is the major drawback of the procedure.
Introduction
An increasing number of male patients present after bariatric surgery with significant deformities: malpositioned nipple–areola, redundant skin, and subcutaneous deficiency, the latter due to subcutaneous tissue depletion. Corrective procedures for grade 3 gynecomastia address problems with skin redundancy similar to those seen in massive weight loss patients.
Simon et al1 published a useful classification of gynecomastia, with grades 1, 2A, 2B, and 3 corresponding to increasing deformity ( Table 23.1 ). The majority of postbariatric patients are placed in grade 3, with marked skin redundancy with or without breast enlargement. In defining the role of suction-assisted and ultrasonic liposuction, Rohrich et al2 developed four grades; the two severe grades, III and IV, are pertinent here ( Table 23.2 ). Grade III exhibits grade I nipple ptosis, whereas grade IV exhibits grade II or III nipple ptosis. The authors advocate ultrasound-assisted liposuction (UAL) with or without staged excision. More than 85% of patients in their series did not require a second open procedure. Only 11% of patients in their series, however, presented with grade IV severity. Song et al3 present a post-bariatric rating scale for breast deformities, but it includes only female patients.
Indications
Surgical management of male chest deformities has evolved to treat all degrees of the condition. The least invasive procedure, liposuction, which is advocated by many authors,4–6 produces excellent results. Rohrich et al2 advocate ultrasonic liposuction as a more efficacious modality for contour correction. It is uncommon that postbariatric patients are candidates for liposuction alone because the redundant skin cannot be addressed. Prior to the availability of liposuction, an open surgical approach was the only option. In 1946, Webster7 described a corrective procedure that employs a semicircular incision within the pigmented areola through which glandular resection is performed. His discussion does not mention problems with redundant skin, even in the large reductions, and he emphasizes the importance of keeping the scar within the areola. Letterman and Schurter8 describe a technique utilizing nipple transposition via an oblique approach initially developed by Dufourmentel and Mouly9 for breast reduction and mastopexy. Here a pedicle bearing the nipple–areola can be moved to the desired position on the chest wall. Pitanguy10 utilizes a transareolar incision for open management. Davidson11 employs a concentric circle method to resect redundant skin, with open resection of excess breast tissue and fat. An oval design is used when nipple elevation is necessary, carrying the nipple–areola on a dermal pedicle. A case report by Silfen et al12 describes an inferiorly based dermal flap to augment the breast and allow nipple–areola transposition. The transposed flap provides volume repletion to the pectoral region. The result illustrated exhibits incorrect nipple position and scars in a nonanatomic position, not in the inframammary fold. Hammond13 utilizes a circumvertical technique when skin excision is necessary. Here a medial inframammary scar is avoided, and the vertical component of the incision reduces periareolar tension seen in the concentric circle technique to achieve less scar hypertrophy and widening. Gusenoff et al14 define pseudogynecomastia as increased amounts of subareolar fat without enlargement of the glandular component of the breast. Many massive weight loss (MWL) patients fit into this category with the additional component of excess skin. The technique utilized in grade 2 gynecomastia by these authors is a thin inferiorly based dermal pedicle, which can be modified to correct the lateral chest and breast deformities. They advocate a free nipple graft procedure for grade 3 gynecomastia. More severe deformities require skin excision in addition to glandular resection.
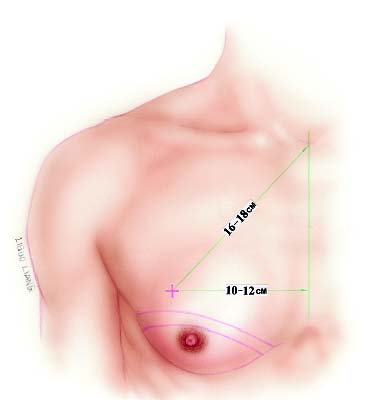
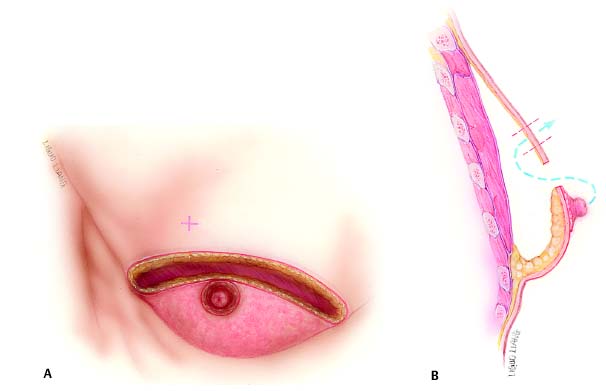
Patients with large breasts and MWL patients have in common a large amount of excess skin that cannot be managed in one stage without an incision beyond the areola. Additionally, the pedicled procedures preserve subareolar volume to achieve appropriate contour. The procedure described in this chapter employs an inferior pedicle similar to the reliable one utilized widely in female reduction mammoplasty. Subcutaneous mastectomy is accomplished to remove excess tissue, preserving the upper flap, which is advanced over the pedicle to the inframammary fold. An opening is cut in the flap to admit the nipple–areola. In addition to providing blood supply to the nipple–areola, the pedicle favorably augments the contour above the inframam-mary fold. MWL patients often display large skin excess that extends laterally to the axilla and arm. The lateral inframam-mary incision can be extended posteriorly to provide skin excision and contour correction in these areas.
Related posts:
 22 Inferior Pedicle Approach for Autologous Augmentation Using the Intercostal Artery Perforator (ICAP) Flap
22 Inferior Pedicle Approach for Autologous Augmentation Using the Intercostal Artery Perforator (ICAP) Flap
 21 Correction of Breast Contour Deformities Using Dermal Suspension and Total Parenchymal Reshaping
21 Correction of Breast Contour Deformities Using Dermal Suspension and Total Parenchymal Reshaping
 20 Superolateral Pedicle for Reconstruction of the Female Breast
20 Superolateral Pedicle for Reconstruction of the Female Breast
 4 Anesthesia and Safety Considerations in the Perioperative Period
4 Anesthesia and Safety Considerations in the Perioperative Period
 17 Brachioplasty with Interdigitation of the Posteromedial Scar
17 Brachioplasty with Interdigitation of the Posteromedial Scar
 36 Facial Rejuvenation: Open Technique
36 Facial Rejuvenation: Open Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


