22 Inferior Pedicle Approach for Autologous Augmentation Using the Intercostal Artery Perforator (ICAP) Flap

Abstract
Reconstruction of the breast and upper body deformities in massive weight loss (MWL) patients can be challenging to the plastic surgeon. Breast ptosis and loss of breast volume plague postbariatric patients. Patients also have excessive lateral axillary and posterior truncal tissue that may require dermolipectomy for correction. We describe a Wise-pattern mastopexy with autologous augmentation designed with a pedicled fasciocutaneous flap based on the intercostal artery perforator (ICAP) to correct breast ptosis, restore breast volume, and eliminate redundant upper truncal tissue. Patients have maintained aesthetically pleasing postoperative results at 12 months. There are minimal complications of infection, wound dehiscence, seroma, or hematoma. Mastopexy with autologous augmentation using the ICAP flap has been found to be a reliable method of breast reconstruction in the MWL patient.
Introduction
Patients who have achieved massive weight loss (MWL) are left with significant areas of redundant skin and subcutaneous tissue secondary to fat atrophy. In particular, the involutional changes of the breast may be a source of distress for the female patient. Loss of breast volume and redundant skin secondary to a tissue expander effect from morbid obesity both contribute to severe breast ptosis after MWL. Furthermore, patients commonly have considerable lateral and posterior tissue surplus of the upper trunk, necessitating an upper body dermolipectomy for the treatment of back rolls.
To reconstruct the upper body deformities in the MWL patient, the areas of the upper back and breast must be addressed. Due to volume loss, standard mastopexy alone is frequently inadequate in reconstructing an aesthetically pleasing breast, and augmentation is required. The “pancake” breasts in MWL patients often provide poor soft tissue coverage to camouflage an implant. Thus, the use of autologous tissue to achieve augmentation has particular utility in this group of patients. The back rolls consist of ptotic lateral axillary and posterior truncal tissue that is supplied by perforators from the thoracodorsal and intercostal arteries; they constitute a potential regional source of tissue for autologous augmentation of the breast. This chapter describes mastopexy with autologous tissue augmentation using a fasciocutaneous flap based on the intercostal artery perforator (ICAP) for the MWL patient. The ICAP flap combined with a Wise-pattern inferior pedicle mastopexy allows reduction of lateral and posterior tissue excess, with restoration of breast volume and contour.
Indications
Patients with MWL and involutional changes in the breast are considered good candidates for this type of procedure. A proper evaluation of skin laxity and nipple position is necessary for proper planning. In addition, excess skin and fat at the lateral chest wall and back rolls are evaluated to determine volume of augmentation. Patients with significant inframammary fold descent, requiring reestablishment of the fold, can undergo this type of a procedure. However, in these cases of inframammary fold descent, a superiorly based breast pedicle in conjunction with ICAP flap augmentation should be considered. Reestablishment of the fold can be difficult with an inferior breast pedicle.
Technique
Planning of the Intercostal Artery Perforator Flap
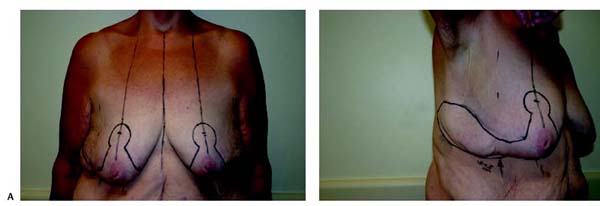
All patients are marked preoperatively in the standing position ( Fig. 22.1 ). A Wise-pattern inferior pedicle mastopexy is outlined as previously described,1 and the ICAP flap is designed as a lateral extension from the mastopexy. The base of the flap is planned along the anterior axillary line and generally measured at 6 to 8 cm in width. A Doppler probe is used to identify cutaneous perforators along the anterior axillary line. The length of the flap is typically 15 to 20 cm, according to the amount of lateral and posterior excess skin and fat. The axis of the flap follows the ribs posteriorly, with a slight superior oblique slant at the distal end ( Fig. 22.2 ).
Surgical Procedure
In all cases, preoperative antibiotics are given. After anesthetic induction, the patient is slightly rotated to prepare the lateral and posterior aspects of the chest wall. In the case of severe back rolls, the patient is placed into the prone position to begin bilateral dissection of the ICAP flaps at their apices. The ICAP flaps are elevated in a posterior-to-anterior fashion, including the muscle fascia. Small perforating vessels from the thoracodorsal branches are encountered lateral to the major intercostal perforators. These small perforators are sacrificed lateral to the level of the serratus muscle. Care is taken to identify and preserve the intercostal perforators located along the lateral chest wall. Primary closure of the flap donor site is performed in a layered fashion using a deep layer of 2–0 Vicryl followed by deep dermal and subcuticular layers of 3–0 Monocryl. Depending on the posterior extent of the excision, a posterior upper body lift can be effectively achieved.
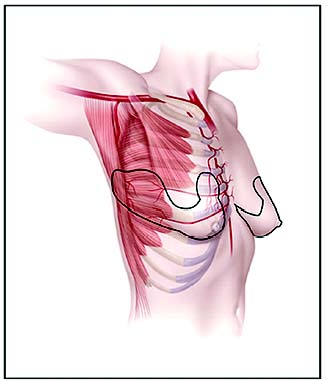
A Wise-pattern inferior pedicle is then de-epithelialized and formed ( Fig. 22.3 ). A subcutaneous pocket is created over the pectoralis muscle fascia up to the clavicle in preparation for the ICAP flap transfer. The intercostal perforators are identified and evaluated with a Doppler probe; they are typically 1.5 to 2 mm in diameter ( Fig. 22.3 ). Care is taken to preserve the perforators within the flap, and further dissection of the vessels through the intramuscular course is often not necessary. After sufficient mobilization of the ICAP flap is achieved, the flap is rotated 90 degrees around the previously created inferior pedicle ( Fig. 22.4 ). Once adequate rotation and positioning are accomplished, the ICAP flap is de-epithelialized. Periodically, the distal tip of the flap is checked for adequate perfusion by sharp excision. A subpectoral saline implant can be used in conjunction with the ICAP flap to obtain additional augmentation. In some instances, the distal tip of the flap is discarded secondary to excessive volume in the reconstructed breast or if tissue perfusion appears clinically suspect.

Related posts:
 23 Breast Surgery in the Male Patient
23 Breast Surgery in the Male Patient
 21 Correction of Breast Contour Deformities Using Dermal Suspension and Total Parenchymal Reshaping
21 Correction of Breast Contour Deformities Using Dermal Suspension and Total Parenchymal Reshaping
 20 Superolateral Pedicle for Reconstruction of the Female Breast
20 Superolateral Pedicle for Reconstruction of the Female Breast
 4 Anesthesia and Safety Considerations in the Perioperative Period
4 Anesthesia and Safety Considerations in the Perioperative Period
 17 Brachioplasty with Interdigitation of the Posteromedial Scar
17 Brachioplasty with Interdigitation of the Posteromedial Scar
 36 Facial Rejuvenation: Open Technique
36 Facial Rejuvenation: Open Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


