21 Correction of Breast Contour Deformities Using Dermal Suspension and Total Parenchymal Reshaping

Abstract
Following massive weight loss, patients are often left with severe breast deformities that present a challenge to plastic surgeons. Traditional mastopexy techniques are often inadequate to correct these contour abnormalities. This chapter presents a technique of dermal suspension and total parenchymal reshaping through an extended Wise pattern. This procedure has the advantage of eliminating the lateral skinfold and using this tissue for autologous augmentation of the breast, obviating the need for a breast implant. Although this technique results in a larger scar burden and longer operative times, it produces a reliable, durable, and safe correction of this difficult problem.
Introduction
Following correction of the abdomen, most women desire correction of their breasts after achieving massive weight loss (MWL). Prior to their weight loss, their breast volume was often full with only mild to moderate ptosis. Unlike patients presenting for traditional mastopexy, these patients often exhibit severe breast deformities.1 The majority of patients presenting for breast recontouring after MWL demonstrate four common problems to varying degrees:
Significant and often asymmetric breast volume loss with grade 2 or 3 ptosis. The breasts often have a deflated and flattened appearance.
Poor skin tone with a severe loss of skin elasticity. There is a high redundant skin-to-breast parenchymal volume ratio.
Medialization of the nipple–areola complex (NAC) in relation to the breast meridian.
Prominent lateral skinfold that blends into the breast. This characteristic is fairly unique to the MWL population. This skinfold often blurs the borders of the lateral breast and the chest wall, forming one continuous roll.
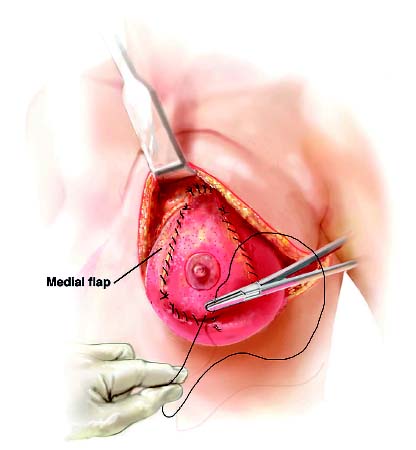
The authors’ preferred technique uses the principles of dermal suspension and total parenchymal reshaping to provide autologous augmentation of the breast and restore superomedial fullness and projection. An extended Wise pattern is created, which allows recruitment of the lateral skinfold to provide the necessary tissue for autologous augmentation. The amount of tissue rotated from the lateral fold can be adjusted to allow for the correction of the breast asymmetry often observed in MWL patients. The entire Wise pattern is de-epithelialized and provides a broad surface that can be suspended to the chest wall at multiple fixation points and can be plicated to provide precise shaping of the breast parenchyma. Short scar techniques, although attractive because of the decreased scar burden, are inadequate to reduce the redundant and inelastic skin envelope in these patients.
Our technique builds upon the work of other plastic surgeons who pioneered the concept of securing the breast tissue to adjacent structures to improve breast shape and projection. Frey2 performed parenchymal reshaping and suspension of a dermal brassiere to the anterior chest wall. Graf and Biggs3 secured an inferior dermoglandular pedicle under a loop of pectoralis and secured it to the pectoralis fascia. Qiao et al4 devised a technique that suspended the parenchyma using dermal fixation to the pectoralis fascia. These suspension techniques provided the basis for our use of dermal suspension and parenchymal reshaping using dermal plication. The use of the redundant lateral skinfold for autologous volume augmentation evolved from Holm-strom and Lossing’s5 lateral thoracodorsal transposition flap for breast reconstruction following mastectomy.
The advantage of this technique is that it provides durable correction of the severe breast deformities seen in MWL patients with a low complication rate. In patients with adequate breast volume, it allows autologous augmentation of the breast parenchyma without the use of a breast implant. Furthermore, the lateral skinfold is eliminated, and this tissue can be used to varying degrees to correct for any breast asymmetry. The main disadvantages of this technique are the increased scar burden and increased operative time required to tailor the exact breast shape. Despite these disadvantages, this technique provides great control of the redundant skin envelope and breast parenchymal shape with long-lasting and reliable results.
Indications
There is great variation in the presentation of breast contour deformities following MWL. Many authors have described different techniques to correct them.6–13 Each consultation must be individualized to correct the particular deformities specific to the patient. Which procedure is chosen depends on several factors: (1) the severity of the aforementioned four contour deformities commonly seen in MWL patients, (2) the desired postoperative breast size of the patient, and (3) the surgeon’s experience. Regardless of which procedure is performed, it must be able to meet the patient’s expectations for size and shape.
The type of procedure performed is mainly dictated by the amount of residual breast tissue and the desired size of the breasts. A small subset of patients present with inadequate breast tissue volume following MWL. These patients are generally younger in age and have very good skin tone. They are good candidates for augmentation mammaplasty with implants. Approximately 20% of patients present with excessive breast tissue volume and are good candidates for breast reduction. Our preferred technique for breast reduction is a superomedial pedicle using an extended Wise pattern, which allows us to better contour the lateral skinfold, if present.
The majority of MWL patients present with adequate breast volume. Patients with mild breast deformities may be good candidates for traditional mastopexy techniques and possibly a short-scar procedure if the skin redundancy is minimal. Existing mastopexy techniques may not be able to correct some of the difficult deformities seen after MWL. Patients who are good candidates for this procedure have the following:
Profound loss of breast volume with flattening of the breast parenchyma
Grade 3 nipple ptosis
Medialization of the NAC
Poor skin tone and an inelastic skin envelope
A prominent lateral skinfold that can be used for autologous augmentation
No desire for breast implants
During the physical examination, a careful evaluation of the remaining breast parenchyma is performed to determine if adequate parenchymal volume is present. During the consultation, the breast tissue is folded upon itself, and the patient is asked if this volume is sufficient. The lateral skinfold is also evaluated to determine the amount of tissue present to augment breast size. In patients with adequate parenchymal volume, a large skin envelope, grade 3 ptosis, medialization of the NAC, and a sufficient lateral skinfold, our preferred method for correction is dermal suspension with total parenchymal reshaping with autologous augmentation using tissue from the lateral skin-fold.6–8 This procedure produces durable results and allows the surgeon to intraoperatively tailor the size and shape of the breast. This technique allows for the correction of difficult asymmetries by allowing varying quantities of tissue to be recruited from the lateral skin roll for autologous augmentation. In some cases, one breast may benefit from this technique, whereas the contralateral side undergoes a breast reduction.
As with any MWL patient who presents to our clinic for body-contouring procedures, a thorough history and physical are performed.14 Specific questions are asked about weight loss history and personal or family history of breast cancer. All patients who are planned for breast surgery undergo mammographic evaluation in accordance with the American Cancer Society’s recommendations.15 A nutritional evaluation is also performed to ensure that the patient is optimized prior to surgery. The patient sent for medical consultation for preoperative surgical clearance as indicated by the patient’s comorbidities.
There are relatively few contraindications to this procedure. Patients who have had previous breast scars that may disrupt the blood supply to the NAC are not good candidates for this procedure. We defer surgery on all active smokers, given the extent of the tissue undermining performed. We ask patients to stop smoking 4 weeks prior to surgery and test all active smokers prior to surgery using a nicotine urine test. Patients with active intertrigo or other severe dermato-logic conditions around the breast are also deferred until the condition is resolved.
Technique
Markings
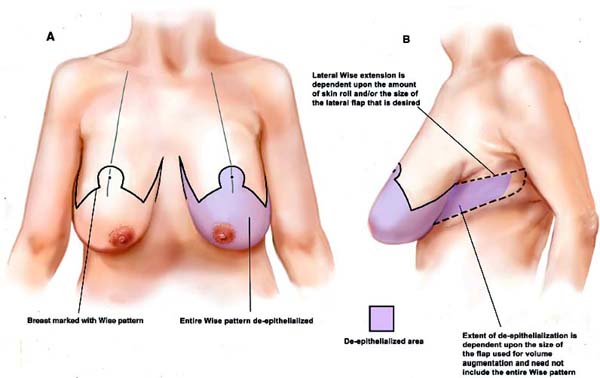
The technique is based on an extended Wise pattern with preservation of both a central and an inferior pedicle ( Fig. 21.1 ). A new breast meridian is symmetrically drawn that ignores the position of the existing medialized nipple. This meridian lies in the middle of the breast and is where the new NAC will eventually be positioned. The new nipple position is referenced to the inframammary fold (IMF) along the breast meridian, and 2 cm is measured cephalad to this point to represent the new height of the NAC. Vertical limbs of the Wise pattern are marked at 5 cm. The lateral markings of the Wise pattern are extended to encompass the lateral skinfold, providing tissue to be used for autologous augmentation of the breast. The Wise pattern can be extended to the posterior axillary line or beyond, depending on the severity of the skinfold to correct the contour of this region. The lateral thoracic perforators provide a robust blood supply to the tissues to be mobilized medially to augment the breast. Despite the adequate blood supply to this region, we generally do not rotate tissue posterior to the posterior axillary line, instead discarding this tissue. Depending on the amount of tissue required to achieve the desire breast size and correct for existing asymmetries, the entire lateral extension can be used, or it can be trimmed.
Related posts:
 22 Inferior Pedicle Approach for Autologous Augmentation Using the Intercostal Artery Perforator (ICAP) Flap
22 Inferior Pedicle Approach for Autologous Augmentation Using the Intercostal Artery Perforator (ICAP) Flap
 23 Breast Surgery in the Male Patient
23 Breast Surgery in the Male Patient
 20 Superolateral Pedicle for Reconstruction of the Female Breast
20 Superolateral Pedicle for Reconstruction of the Female Breast
 4 Anesthesia and Safety Considerations in the Perioperative Period
4 Anesthesia and Safety Considerations in the Perioperative Period
 17 Brachioplasty with Interdigitation of the Posteromedial Scar
17 Brachioplasty with Interdigitation of the Posteromedial Scar
 36 Facial Rejuvenation: Open Technique
36 Facial Rejuvenation: Open Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


