21. Botulinum Toxin
Definition
Botulinum toxin is a neurotoxin that is produced by Clostridium botulinum, a gram-positive anaerobic bacterium.
History and Physiology
Botulism
The toxin was identified as the cause of a symmetrical, neuroparalytic illness.
Foodborne botulism occurs from the ingestion of the neurotoxin and rarely occurs in the modern era, except in home-canned goods or rare instances.
Wound botulism occurs when the bacteria colonize a wound and produce the toxin, causing progressive weakness.
Infant botulism—the most common in the United States (100 infants/year)—results from the ingestion of clostridial spores, colonization of the gut with the bacteria, and production of toxin.
Toxins
Clostridium botulinum produces eight toxins, of which seven have paralytic properties: serotypes A through G.
Antigenetically distinct with different sites of action 4
Mechanism of action
The neurotoxin acts at presynaptic nerve terminals to inhibit the release of acetylcholine, producing a chemodenervation.
The protein consists of a heavy and light chain. The heavy chain irreversibly binds to the nerve terminal, and the toxin is internalized through endocytosis, where it renders the nerve terminal nonfunctional and blocks the release of acetylcholine into the neuromuscular junction. 4
It targets the SNAP/SNARE docking protein complex and the vesicle-associated membrane protein (VAMP) (type B toxin).
Recovery is through two phases:
Phase 1: Accessory terminals sprout from the affected axon to stimulate the postsynaptic target.
Phase 2: After 28 days, the main axon teminal begins slow recovery of its acetylcholine release ability. At appromately 90 days recovery is complete. 4
Type A was purified in crystalline form in 1946.
In the 1970s type A was first used clinically in treating strabismus and then facial dystonias.
Carruthers and Carruthers 5 then described the first aesthetic use of toxin for the treatment of glabellar frown lines in 1992.
Types A and B are FDA approved for clinical use.
Type A is approved for multiple clinical uses, including the cosmetic improvement of glabellar rhytids and crow’s-feet in patients 65 years or younger.
Expanded to include hyperhidrosis, blepharoptosis, and cervical dystonia.
Type B is approved for cervical dystonia.
Three preparations of type A are available for facial cosmetic use (Table 21-1).
Indications and Contraindications
Indications
Despite limited FDA approval, widely used off-label to improve dynamic facial rhytids
Contraindications
Active infection at the proposed injection site
Known hypersensitivity to any ingredient in the formulation, including albumin
Precautions
Botulinum toxin is used cautiously in:
Patients with neuromuscular disorders including ALS, myasthenia gravis, and Lambert-Eaton syndrome, because they may have significant side effects
Coadministration with aminioglycoside antibiotics or other agents that interfere with neuromuscular transmission, which can potentiate the effect of type A toxin
Pregnant women (category C): Adverse effects shown in animal pregnancy studies, but inadvertent use has not resulted in problems in humans
Lactating patients, as it is unknown whether the toxin is excreted in human milk
Inflammatory skin conditions are the site of planned injection
Patient Evaluation
History
Age
Gender
Medical comorbidities
History of prior treatments and preferences
NSAID use and other medications (may increase bruising)
Analysis
Evaluate static and dynamic rhytids in the upper and lower face.
Identify platsymal bands.
Assess brow symmetry and aperture width.
Identify any preexisting brow or upper lid ptosis.
Other Considerations
Skin quality: More toxin is generally required for thicker skin.
Muscle mass: Male patients tend to have larger facial muscles and require more toxin.
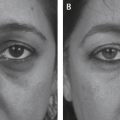
Photographs
Static and dynamic (animated) preprocedure photographs are helpful, especially for patients not previously treated.
Patient Expectations
Patients have varying desires for treatments. Some request near-complete denervation, whereas others prefer a more limited treatment.
Static lines frequently soften, but they are rarely eliminated. Treatment improves dynamic rhytids.
Longevity is approximately 3 months on average, but varies by dose, muscle bulk, and injection site.
Tip:
In patients who have had prior treatments, a history including results and preferences is especially important.
Informed Consent
The risks, benefits, and alternatives to the procedure need to be presented. The planned injection sites may not be FDA-approved indications and are considered off-label use.
Recommended items to be included in the informed consent:
A general description of the procedure and location of injections
A sufficient description of potential risks
Pain at injection site
Bleeding
Bruising
Eyelid or brow ptosis
Headache
Allergic reaction
Nausea
Facial asymmetry
Dysphagia
Respiratory compromise
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


