20 Superolateral Pedicle for Reconstruction of the Female Breast

Abstract
Reshaping of the breasts is an important stage in body contouring of the massive weight loss patient, as the breasts generally undergo marked change after weight loss and, as a result, are an area of major concern to the majority of patients. Existing breast surgery techniques need to be tailored to the unique needs of this subset of patients. Prior to weight loss, the breast tissue expands with large amounts of fatty tissue. To nourish this fat, an extensive amount of circulation develops. When the fat is lost, much of the microvasculature remains. On the basis of this increased vasculature, longer pedicles of breast tissue can be fashioned to provide a redistribution of breast volume and an “autologous augmentation” of the breast. With particular consideration of the primary pattern of sensory innervation to the nipple–areola complex, the authors have utilized the superolateral dermoparenchymal pedicle as a basis for surgery on a variety of presenting breast shapes in weight-loss patients, adapting the technique to successfully address the specific anatomic challenges encountered. This has been proven to be a versatile and effective technique for a wide array of breast morphologies and with different patterns of skin excision. The operative technique involves superior rotation of a superolaterally based dermoparenchymal pedicle, resulting in a “periwinkle” effect that provides desirable superior pole fullness and increased projection to the breast, as well as the ability to create autologous augmentation of the superior pole using the patients’ own breast tissue. Experience has demonstrated that the operation is safe, effective, and aesthetically pleasing.
Introduction
The number of bariatric procedures being performed in the United States is rapidly rising. After the massive weight loss that occurs following these procedures, patients are left with significant contour deformities involving the abdomen, breasts, arms, thighs, and face. Although much has been written about improving abdominal contour in this subset of patients, the literature addressing management of the breast in these patients remains sparse.
The majority of patients who have experienced massive weight loss request breast surgery. The goals of breast-contouring surgery in this subset of patients are the same as those applied to the general population, including correction of ptosis, reduction or augmentation of volume, improvement in shape with increased superior pole fullness, and maintenance of a sensate and viable nipple–areola complex. Although an acceptable result can be obtained in some patients using the numerous standard techniques of breast reduction and mastopexy that have been described,1–6 these techniques do not address certain problems that are specific to many of the patients who have undergone massive weight loss. Unique considerations include the often poor elasticity of the skin and tendency for recurrent ptosis, severe loss of breast volume, thin breast flaps, and extension of the lateral breast fold. The lateral breast fold usually is quite prominent in these patients and often extends far posteriorly onto the back into a superior back roll. Therefore, standard techniques need to be altered in massive weight loss patients to achieve the optimal result.
Indications
Almost all patients require elevation of the nipple–areola complex in the form of a mastopexy. Several authors have demonstrated the safety of mastopexy, either alone or in combination with other body-contouring procedures.7–10 However, mastopexy techniques in this population are still evolving. Rhomberg et al7 have described modifications of standard mastopexy techniques to meet the requirements of these patients. A variety of pedicles for nipple–areola transposition have been described, including use of the standard inferior pedicle reduction.11
We have previously described our experience with the superolateral dermoparenchymal pedicle for a wide range of breast surgery applications and have created a classification system that assists in patient selection:12
Type I: Superolateral dermoparenchymal pedicle using the modified Wise pattern1
Ia: Reduction mammaplasty of 1200 g per patient or more
Ib: Mastopexy for ptosis with minimal to no reduction of breast parenchyma
Ic: Reduction mammaplasty with free nipple graft
Type II: Superolateral dermoparenchymal pedicle using the vertical pattern
IIa: Reduction mammaplasty of 1200 g per patient or less
IIbi: Mastopexy for ptosis
IIbii: Mastopexy for ptosis with mammary prosthetic implant
The anatomic innervation to the breast has been described by several authors. A detailed description of the anatomy was provided by Sir Astley Cooper13 in 1840. Craig and Sykes14 have elucidated the importance of the third, fourth, and fifth anterior cutaneous nerves, and the fourth and fifth lateral cutaneous nerves, in supplying sensation to the nipple–areola complex. Courtiss and Goldwyn6 identified the lateral cutaneous branch of the fourth intercostal nerve as the major source of innervation to the nipple–areola complex. Attempts at preserving maximal nipple–areola sensation during breast surgery should take these anatomic features into account.
The superolateral dermoparenchymal pedicle technique has evolved from several other operations, including the Strombeck15 horizontal bipedicled dermoparenchymal flap and the Skoog16 lateral dermal pedicle. Nicolle17 has presented his experience with the lateral dermoparenchymal pedicle for breast reduction, and Cárdenas-Camarena and Vergara18 have described use of the superolateral dermo-glandular pedicle.
The superolateral pedicle can be employed with different patterns of skin excisions, including vertical excision and modified Wise-pattern excision. Patients with extensive lateral breast folds have been shown to benefit more from a modified Wise-pattern excision, as the transverse incision can be extended along the lateral breast and chest wall, extending into the lateral chest and back roll for greater correction of this deformity. Younger patients with better skin tone and patients undergoing augmentation mastopexy may be candidates for a vertical pattern excision in combination with implant placement, as the increased projection of the skin and glandular envelope afforded by the prosthesis may improve the lateral breast contour. Improved superior pole fullness may be achieved by maintaining continuity of the pedicle with the inferomedial breast parenchyma, rotating and folding the excess tissue superiorly with the pedicle to provide an autologous augmentation of the upper pole. The most frequently used techniques in the massive weight loss population are the Ib, IIbi, and IIbii types.
Technique
The technique used is the Wise-pattern procedure ( Fig. 20.1 ).
Markings
The preoperative skin markings are drawn with the patient in the standing position. A modified Wise pattern is utilized. The breast meridian is determined as follows. The distance from the sternal notch to the acromion is measured along the clavicle. From the midpoint, a vertical line is drawn, separating the breast mass equally. This line is generally toward the nipple–areola complex, unless the complex is severely displaced.
Markings for nipple placement are made along the breast meridian at a level that accounts for the patient’s breast size and shape, height, and degree of nipple ptosis. Nipple placement is generally located between 21 and 25 cm from the sternal notch along the vertical line. The Wise pattern is centered over the nipple placement site and drawn with indelible ink marker. The inframammary fold is marked to include the excess fold laterally to the anterior axillary line. From the lower points of the vertical line, a line is drawn laterally and medially to intersect with the inframammary line. In this manner, the excess fold laterally will be excised.
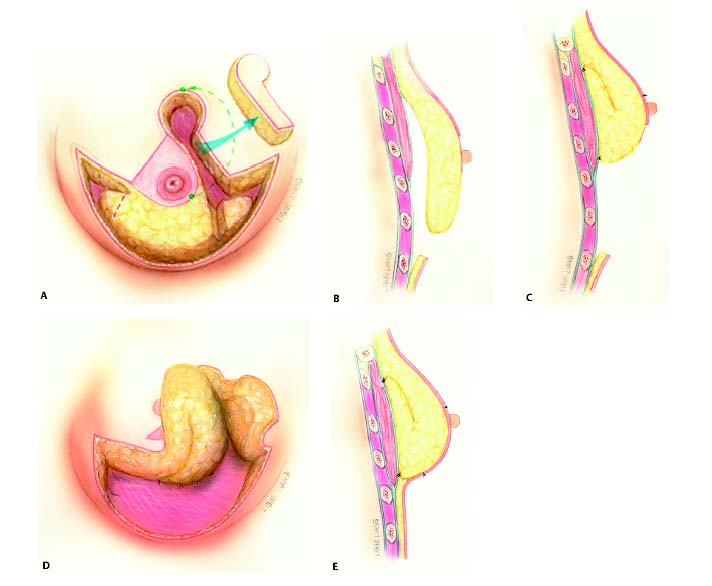
Pedicle Creation
With the patient anesthetized in the supine position, a tour-niquet is placed at the base of the breast. The areola is traced with a 42 mm-diameter washer, centering the nipple in the hole of the washer. The superolateral dermoparenchymal pedicle is then drawn with a 10 to 12 cm width, starting 2 cm lateral to the meridian and ending 2 to 3 cm lateral to the lower edge of the lateral point of the vertical marking. A 1:1 ratio of length/width of the pedicle is the result. Contiguous parenchyma distal to the end of the pedicle already marked is now outlined. When this additional parenchyma is folded under the dermoparenchymal pedicle and sutured to the pectoralis major muscle, it serves as an autologous augmentation of the upper pole.
In type Ia patients (reduction and nipple–areola transposition), the breast resection is accomplished with incisions perpendicular to the chest wall, following the Wise pattern, excising excess skin, breast, and fat to the level of the pectoralis major fascia. Patients with exceedingly large breasts are considered candidates for the superolateral pedicle with a free nipple graft (type Ic). As a general rule, this latter procedure is used in cases in which the distance from the nipple to the sternal notch exceeds 40 cm preoperatively. In these cases, the superolateral pedicle is drawn, ignoring the significantly lower nipple–areola complex. The entire pedicle is de-epithelialized. Creation of the pedicle is then performed as in a standard reduction, by incising at the borders of the pedicle to the level of the pectoralis major fascia. The nipple–areola complex, having been removed initially, is thinned to a thick split-thickness graft and then suture- bolstered to the rotated de-epithelialized pedicle. In the pure mastopexy cases (type Ib), the breast tissue that otherwise would have been resected during a reduction mammaplasty is similarly maintained in continuity with the superolateral dermoglandular pedicle, after removal of the full thickness of the overlying skin.
Related posts:
 22 Inferior Pedicle Approach for Autologous Augmentation Using the Intercostal Artery Perforator (ICAP) Flap
22 Inferior Pedicle Approach for Autologous Augmentation Using the Intercostal Artery Perforator (ICAP) Flap
 23 Breast Surgery in the Male Patient
23 Breast Surgery in the Male Patient
 21 Correction of Breast Contour Deformities Using Dermal Suspension and Total Parenchymal Reshaping
21 Correction of Breast Contour Deformities Using Dermal Suspension and Total Parenchymal Reshaping
 4 Anesthesia and Safety Considerations in the Perioperative Period
4 Anesthesia and Safety Considerations in the Perioperative Period
 17 Brachioplasty with Interdigitation of the Posteromedial Scar
17 Brachioplasty with Interdigitation of the Posteromedial Scar
 36 Facial Rejuvenation: Open Technique
36 Facial Rejuvenation: Open Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


