20 Backward Extraction-Reposition Technique of Quadrangular Cartilage
Summary
Surgical repair of septal perforations represents a complex technical challenge for the surgeon. Many different surgical techniques have been proposed for the closure of septal perforations, but there is no standard protocol universally accepted. The Cottle technique is a viable procedure for the closure of small- and middle-sized perforations. We here present our experience, using the Cottle technique with the backward extraction-reposition of nasal septum and inverted sliding flap suture technique. A fundamental prognostic indicator of successful surgery is the amount of septal structures remaining within the rest of the septum. An important surgical success factor is the surgeon’s experience and skill. Correction of concomitant nasal deformities improves functional results and patient satisfaction; the reduction in flow turbulences avoids drying of the mucosa and consequently the risk of reperforation.
20.1 Indication
Symptomatic small- to medium-sized perforation
20.2 Surgical Anatomy and Operative Implications
Nasal septal perforations (NSPs) are anatomical defects of nasal septum caused by the necrosis of the cartilage and/or bone tissues and their mucous covering. Perforations are classically distinguished according to their etiopathogenic factors, size, and location. 1 , 2 , 3 Size and location must be considered because they determine the choice of the reconstructive procedure and consequently the closure rate success. For this purpose, some basics of anatomy should be considered by the surgeon to discriminate the amount and the type of tissue defect, whereas the knowledge of septal vascularization is essential for the planning of the endonasal flaps.
The nasal septum divides the nose into two cavities. The bony components of the septum include the nasal crest of the palatine bone, nasal crest of the maxilla and premaxilla, vomer, perpendicular plate of the ethmoid, nasal crest of the frontal bone, and spine of the paired nasal bones. The anterior septum is composed of the quadrilateral cartilage and joins the free edges of the aforementioned bones. The anterior superior margin of the quadrangular cartilage joins, at its extreme cephalic, with the caudal end of the median suture of nasal bones contributing, together with the ethmoid perpendicular plate and the upper lateral cartilages, gives the support of the nasal vault. The anterior superior angle of the septal cartilage, defined as septal angle, constitutes an important surgical point. The septal angle is located immediately above the lower lateral cartilages in the supratip area. The loss of cartilaginous support in this area can cause the collapse of the mid-nasal vault. The caudal margin goes from lobule to the nasal spine, contracting relationships with the membranous septum. The caudal edge presents an intermediate angle and a posterior angle just above the nasal spine.
The osteocartilaginous skeleton is covered by periosteum and perichondrium, which are highly vascularized. The arterial blood supply consists of terminals from the external and internal carotid systems. 4 The sphenopalatine artery, terminal branch of the internal maxillary artery (external carotid artery), gives rise to outer branches such as the artery of the middle turbinate and the artery of the inferior turbinate, and also internal branches such as the septal artery that gives rise to the artery of the upper turbinate and septal arteries.
All these arteries anastomose with the ethmoid arteries. The underseptal artery, branch of the facial artery, runs along the nasal vestibule region and the lower anterior septal cartilage. The anterior ethmoid artery, branch of the ophthalmic artery (internal carotid), gives rise to two branches: an internal nasal and external nasal branches, which supply the frontal sinuses and ethmoid cells. The internal and external posterior ethmoidal arteries have anastomose with the anterior ethmoidal artery at the level of the turbinates and with the sphenopalatine artery in the upper part of the septum.
20.3 Patient Selection
Surgical repair of septal perforations represents a complex technical challenge for the surgeon. The principal aims of the surgery are to repair the mucous and also to reestablish the function and physiology of the nose. 5 Many different surgical techniques have been proposed for the closure of septal perforations, but there is no standard protocol universally accepted. 6 , 7 , 8 , 9 , 10 This multitude of different techniques suggests that there is no better procedure than another, but several factors play a role in both decision making of surgical planning and treatment success. 11 A fundamental prognostic indicator of successful surgery is the amount of septal structures remaining within the rest of the septum. An important surgical success factor is the surgeon’s experience and skill. Another critical factor is the adequate view of the operative field, and thus the collaboration of the anesthesiologist is essential to achieve an effective haemostasis. All the techniques are also variably associated with a number of different grafts, both autologous and heterologous, to obtain a safer closure. 12 , 13 More recently, some authors have developed the endoscopic approach to improve visualization without performing an excessive dissection. 14 , 15 , 16 , 17 , 18
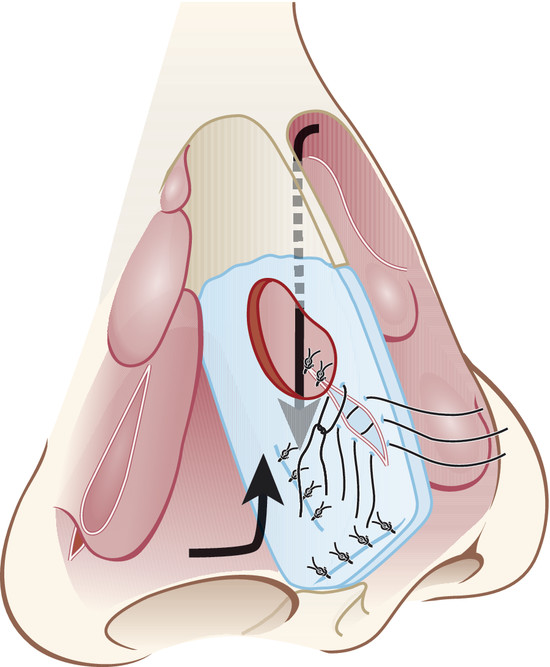
In case of small- to medium-sized perforation, the endonasal approach is the treatment of choice. The backward extraction-reposition technique allows the defects of cartilage and mucoperichondral-mucoperiosteal coating to be situated on two different levels, making safer the strength of the suture of the flap. 19 A further safe point is also provided by the inverted sliding flap suture (Fig. 20‑1). This asymmetric movement of flaps enables a nonopposing suture line and a better mucoperichondral blood supply to the repositioned graft. 20 The endonasal approach, compared with open techniques, enables a small incision, without sacrificing tissues or structures for improving the exposition. We must consider that any incision is bounded to undergo some degree of contraction after surgery, so it is more convenient to perform the lowest number of incisions, above all in this type of surgery. Furthermore, many perforation repair procedures often require the use of interpositional autografts between the repaired flaps and they are consequently accompanied by donor site morbidity. Contrarily, this technique, by repositioning the remaining nasal septum, does not require further supporting implants and that way allows the perforation to be closed without associated morbidity.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


