2 Presurgical Treatment
Introduction
The principal goal of presurgical treatment of an infant with cleft lip and palate is to reduce the severity of the cleft deformity with the intent of improving the outcome of the primary surgical repair. Since the 17th century, various treatment modalities have been pioneered and have been collectively termed presurgical infant orthopedics (PSIO). Although initial efforts were guided by the desire to retract the protrusive premaxilla with an extraoral appliance, they did little to address the alveolar segments. It was not until the 1950s when McNeil first described the intraoral molding plate designed for preoperative reduction of the width of the palate.1 The appliance was fraught with two primary shortcomings: lack of appropriate retention of the appliance and the inability to generate sufficient force to achieve desired results. In 1975, Georgiade and Latham developed a pin-retained appliance to simultaneously expand the posterior alveolar segments while also retracting the premaxilla in patients with bilateral cleft lip and palate.2 Latham subsequently introduced a similar pin-retained appliance for patients with unilateral cleft lip and palate.3 It was also during this time that Hotz described the use of a passive orthopedic plate to slowly align the cleft segments.4–6 The appliance came to be known as the Zurich appliance. Although these are all appliances, lip adhesion surgery7 and lip taping8 have been shown to effectively reposition the alveolar segments as well.
Although many of these methods were and continue to be used in various cleft centers worldwide, they came under much scrutiny following published data primarily from the Dutch Intercenter Study (Dutchcleft). The studies sought to analyze the effects of PSIO treatment in complete unilateral cleft lip and palate. From these studies, it was concluded that there is not a significant long-term benefit of PSIO treatment with speech, nutritional status, dental relationships, or nasolabial esthetics, and that the benefits of PSIO appliance therapy are only seen during the first few years, if at all.9–14 It is important to recognize that all of the Dutchcleft studies that support these conclusions used only the passive Zurich appliance, whereas other studies used a passive and active appliance with the same results.15,16 Guided by these multicenter studies, PSIO therapy had largely fallen out of favor at several centers.
Although the common thread in the described modalities is the ability to reposition the alveolar segments, none address the primary nasal deformity in cleft lip and palate. The severe nasal deformity associated with cleft lip and palate is often the most noticed manifestation of this condition. Patients commonly undergo numerous secondary surgical attempts during childhood to correct the nasal deformity. With each surgical intervention, there are the consequent scars and impact on growth of the surrounding structures.
The concept of being able to alter the nasal form has its origins in work described by Matsuo, where he showed that infant auricular cartilage has the ability to be molded.17 Taking cues from the unique plasticity of neonatal auricular cartilage, a custom intranasal stent was developed to mold nasal cartilage. The appliance, however, was limited in its application because it required an intact nasal floor for retention and did not address the alveolar defect.18 It was not until the advent of nasoalveolar molding (NAM) therapy in the early 1990s by Grayson that there was an appliance that not only enabled effective approximation and alignment of the lip and alveolar segments, but, more importantly, corrected nasal cartilage asymmetry and increased columella length.19–21 Since the introduction of the NAM appliance, the field of PSIO has been reinvigorated because, unlike other forms of PSIO, NAM therapy has the unique ability to change nasal shape and form. It has been adopted by many cleft centers and there is now growing evidence of the benefits of NAM22 in both unilateral cleft lip and palate (UCLP)23 and bilateral cleft lip and palate (BCLP).24
This chapter focuses on the use of NAM for the presurgical management of an infant with either BCLP or UCLP. The chapter also highlights clinical pearls and potential pitfalls associated with NAM therapy. Finally, an algorithm is offered in order to inform the rationale for various decision points while performing NAM therapy, and an evidence-based medicine statement about the use of NAM is included.
Goals of Nasoalveolar Molding Therapy
The chief objective of NAM is to reduce the severity of the unilateral or bilateral cleft and alveolar and nasal deformities prior to the primary reconstructive surgery so as to optimize the clinical outcome. In the case of UCLP, the columella, which is characteristically deviated toward the unaffected side, is straightened. Also, the cleft-side lower lateral alar cartilage, which is prolapsed and concave, is supported and molded to a more symmetric, convex form ( Fig. 2.1 ). In the case of BCLP, the ability to nonsurgically elongate the columella, achieve forward projection of the nasal tip, and align the premaxilla is invaluable in producing a better esthetic outcome ( Fig. 2.2 ).

NAM Appliance
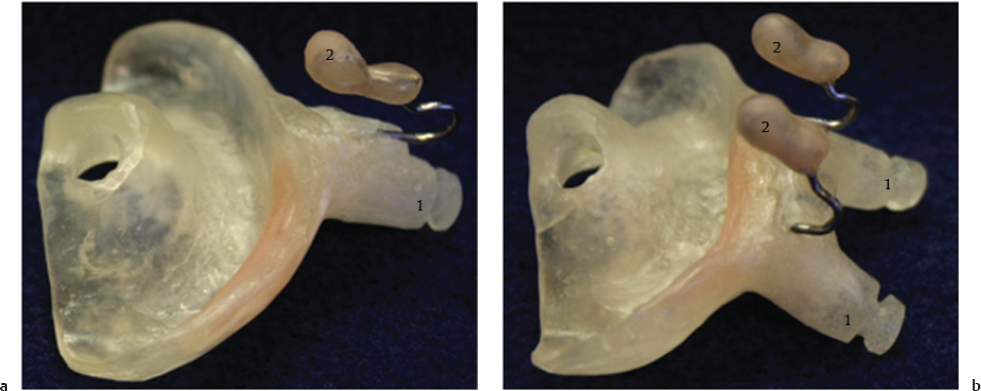
The NAM appliance has both an oral and nasal component. The acrylic alveolar molding plate serves to mold the cleft alveolar segments and bring them into closer proximity. The nasal stent portion of the appliance is composed of acrylic and wire, and molds the distorted nasal cartilage of the affected side in order to make it symmetrical with the unaffected side in a unilateral cleft, or both affected sides in a bilateral cleft. The retention buttons are acrylic extensions on the anterior aspect of the appliance, which, in combination with the retention tapes, serve to secure the appliance in the mouth. The appliance is modified on a weekly basis for approximately 3 to 4 months in the case of UCLP and 4 to 6 months for BCLP ( Fig. 2.3 ).
The Decision to Undergo NAM Therapy
NAM therapy is a labor-intensive endeavor on the part of the family who has a newborn with cleft lip and palate. It can be an overwhelming time in their life, and the capacity of the cleft team to provide support through this period is critical. Ideally, the family would meet with members of the cleft team prenatally if the cleft is identified in utero, or otherwise soon after the infant is born. This would aid the family in receiving support for caring for an infant with a cleft and, moreover, it would establish expectations for NAM therapy. This includes regular weekly or biweekly visits for adjustments of the appliance, as well as the commitment that it takes at home to clean the appliance and apply the indicated retention tapes. In order to provide a broad and realistic understanding of the caregiver′s role in NAM therapy, the team can facilitate contact with other families who have had children who have undergone NAM. Once the family is made aware of all that NAM therapy entails, and the alternatives, they can make an informed decision about whether to pursue treatment. Should the family decide to not pursue NAM therapy, they are often encouraged to apply cross-cheek tapes. A recent article by Sischo et al. reported that NAM is offered by just over one-third of U.S. cleft teams.25

Diagnosis and Treatment Plan
A thorough examination of the infant by the surgeon, orthodontist, and other team members will guide the formulation of an individualized set of treatment objectives. They are influenced by age of the infant, type and severity of the cleft, presence of a Simonart′s band, presence of a tooth bud erupted in the cleft margin, and other remarkable findings. NAM therapy is ideally initiated early in the neonatal period (within the first month after birth) to facilitate appliance acceptance and to take advantage of nasal cartilage plasticity. In the case of an infant older than 3 months, the ability to mold the tissues is difficult, as is the baby′s acceptance of the appliance. The parents should be made aware of the potential difficulties prior to initiating treatment.
The type of cleft can influence the sequence of treatment. In severe cases of BCLP where the premaxilla is considerably ectopic and protrusive, the best course may be to pursue taping prior to obtaining impressions for the appliance. The nasal deformity can be every bit as severe in incomplete cleft cases, providing indication for the use of NAM when appropriate. When a Simonart′s band is present, it is usually serving to facilitate the goals of NAM, but on occasion, if its points of attachment work counter to approximation of the alveolar cleft, it can be cut. If there is a neonatal tooth that is not supported by bone or erupted on the cleft margin, extraction is often indicated to minimize the potential for aspiration or interference with approximation of the alveolar segments. The comprehensive examination, coupled with an individualized treatment plan, sets the stage for establishing expectations of treatment, as well as optimizing treatment outcomes.
Lip Taping (Prior to NAM)
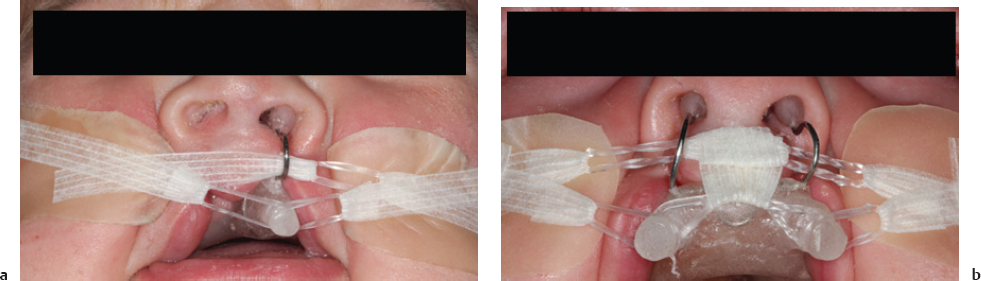
In the time preceding insertion of the NAM appliance, parents are often encouraged to initiate lip taping. The rationale for beginning prior to appliance delivery is twofold: (1) it initiates the process of reducing the size of the alveolar cleft and interlabial gap(s); and, more importantly, (2) it allows both the infant and parents to become accustomed to using the lip tapes, as they will be maintained throughout NAM therapy. In both UCLP and BCLP, a hydrocolloid base tape is applied to both cheeks. For UCLP, two quarter-inch Steri-Strips (3M; St. Paul, MN) are connected with an orthodontic elastic between them. The constructed tape is then placed from the noncleft side to the cleft side under tension, with the elastic being positioned between the lip segments. For BCLP, two elastics are used with a central Steri-Strip between the two elastics and one Steri-Strip to be taped to each cheek. The central Steri-Strip can be surrounded by a strip of base tape and positioned over the prolabium. This is shown in Fig. 2.4a for UCLP and Fig. 2.4b for BCLP.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


