2 Concepts for Surgical Treatment—Procedure Navigator
Aims of Treatment
The female breast is the site of a number of functional and morphological disorders that are treated primarily by surgery. The treatment of breast cancer, the commonest malignant disease in women in the Western world, dominates breast surgery. Esthetic aspects are particularly important as the breast is such a fundamental organ for a woman’s subjective self-image, in both “esthetic surgery,” which focuses on the cosmetic aspects, and in “reconstructive esthetic surgery” after an operation for breast cancer. The following procedure navigator describes the most important clinical situations with the appropriate surgery. In addition, the complex area of oncoplastic surgery is defined and described in detail, identifying suitable patients for the various surgical approaches.
Anatomic–Morphologic Procedure Navigator
Functional Diseases Mastopathy – Fibrocystic Mastopathy
In recent years, the nonspecific term “mastopathy” has been superseded by clear histological diagnoses for which specific surgical or watch-and-wait treatment concepts have been developed. Mastopathy describes fibrous and glandular changes in the breast, sometimes with a proliferative appearance, diagnosis of which is particularly important to distinguish it from (intra-) ductal and lobular neoplasia (DIN, LIN). “Mastopathy” classically signifies benign, fibrotic, and cystic fibrotic areas of the breast associated clinically with mainly premenstrual pain, induration, and recurrent cysts; it may be apparent on imaging (ultrasonography, mammography) as nonhomogeneous areas of tissue and microcalcifications.
After imaging has shown the extent of the condition, the diagnosis can be confirmed by biopsy (fine needle aspiration, core cut biopsy, vacuum biopsy). Aspiration of large troublesome cysts can alleviate symptoms and facilitates cytology.
Surgical Repertory
Core biopsy, vacuum biopsy p. 31
Simple lumpectomy p. 34
Operation of Choice
Confirmation of benign histology and symptomatic treatment

Functional Diseases Mastopathy – Duct Ectasia
Duct ectasia is dilatation of the lactiferous ducts that is without pathological significance and is not precancerous, but it is occasionally identified as the cause of pathological secretion. Galactography aids diagnosis and exact localization of the secreting duct and any lactiferous duct papillomas or ductal carcinoma in situ (DCIS). The new technique of ductoscopy has not yet become established. Treatment is aimed at correcting the secretion and excluding a proliferative process with certainty. Complete removal of the lactiferous duct system may be indicated in the case of multiple or recurrent symptomatic duct ectasia (retroareolar segment, Urban operation).
Surgical Repertory
Ductectomy after intraductal patent blue p. 38
Ductoscopic marking and resection p. 38
Retroareolar segmental resection (Urban operation) p. 38
Operation of Choice
Ductectomy after intraductal patent blue
Functional Diseases Mastopathy – Nipple Discharge
A distinction can be made between physiological and pathological secretion or galactorrhea depending on whether one or both breasts are affected and on whether the secretion is bloody, serous, or milky. The differential diagnosis includes hormonal, functional, and morphological disorders. Papillomas without atypia are benign intraductal epithelial tumors without malignant potential. An intraductal papilloma is the most frequent cause of a bloody pathological secretion. Galactography plays an important part in diagnosing papilloma and other causes of nipple discharge. Ductoscopy is an alternative. Excisional surgery or complete removal with the vacuum-assisted biopsy system is indicated when an intraductal papilloma is suspected, if duct ectasia is found, and, rarely, because of persistent secretion after failure of all conservative treatments.
Surgical Repertory
Ductectomy after intraductal patent blue p. 38
Ductectomy after ultrasound-guided wire marking p. 38
Retroareolar segment p. 38
Operation of Choice
Ductectomy after intraductal patent blue

Functional Diseases Inflammation – Puerperal Mastitis
Puerperal mastitis is one of the most common complications of childbirth. As a result of incomplete emptying of the lactating breast (engorgement) due to inadequate suckling or overproduction, milk leaks into the periductal connective tissue, producing a local inflammatory reaction. The next stage is superinfection by skin bacteria from the nipple (> 90% staphylococci). Without adequate early treatment, there is a risk that the disease will progress to a breast abscess. The most important steps in treatment therefore consist of draining the breast as soon as possible, pumping in addition to breast-feeding, and cooling the breast to reduce the volume of milk produced subsequently. Antibiotics do not solve the underlying problem but help when superinfection is already present. Treatment is surgical only at the abscess stage with ultrasound-guided fine needle aspiration or incision and drainage. If necessary, milk production can also be limited by drugs.
Surgical Repertory
Abscess aspiration, aspiration to exclude abscess p. 42
Surgical abscess drainage p. 42
Operation of Choice
Surgical abscess drainage

Functional Diseases Inflammation – Nonpuerperal Mastitis
Nonpuerperal mastitis is rarer and its clinical presentation is more varied. A breast abscess not associated with pregnancy or lactation usually occurs in the central region of the two lower quadrants. The average age of the patients is greater than with puerperal mastitis. Apart from smoking, predisposing factors include hyperprolactinemia, pre-existing fibrocystic disease, diabetes mellitus, thyroid dysfunction, and use of certain psychotropic medications.
Exclusion of a co-existing breast cancer is crucial in the diagnosis and treatment of nonpuerperal mastitis, which must be distinguished with certainty from inflammatory breast cancer or Paget’s disease. After surgical drainage, the disease course can be prolonged with recurrence and fistula formation, especially in heavy smokers or immunosuppressed patients.
Surgical Repertory
Abscess aspiration p. 38
If the diagnosis is in doubt or condition persists: punch biopsy of the skin p. 31
Surgical abscess drainage p. 38
Fistula excision p. 38
Counterincision for drainage p. 38
Operation of Choice
Surgical abscess drainage
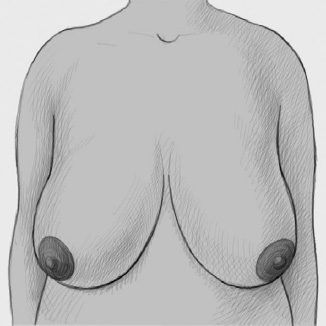
Functional Diseases Esthetic Problems – Macromastia
Breasts regarded by the patient as too big are mainly a functional problem in Northern Europe and North America, when macromastia is present objectively and associated with problems such as intertrigo, poor posture, furrows caused by the bra, and chronic pain, especially in the shoulders and back. In Latin America, even normal-sized breasts are reduced for esthetic reasons, which is why some modern breast reduction techniques were developed in this region. The suffering of patients with severe macromastia is considerable and most patients are very happy with the postoperative result.
Surgical Repertory
Central pedicle p. 96
Centroinferior pedicle p. 96
Superior pedicle p. 96
(Strömbeck reduction mammoplasty) p. 96
McKissock reduction mammoplasty p. 96
Operation of Choice
The operation of choice depends essentially on the reduction volume, the patient’s age, and additional risk factors for nipple management:
Very large breast—high risk: centroinferior pedicle over inverted T
Medium-sized breast—normal risk: central pedicle through periareolar approach or superior pedicle
Functional Diseases Esthetic Problems – Micromastia
The medical significance of excessively small breasts derives from the mental stress they cause the patient, which can vary greatly depending on her personality and ethnic and cultural background. Surgical treatment consists of augmentation mammoplasty using a breast implant. Implants come in many forms, either modern silicone gel pads or saline-filled implants. The procedure is generally regarded as purely cosmetic. However, there are also special cases and extreme cases where there can be little doubt about the purpose of surgery even if the old principle of cosmetic surgery, “surgery not of the body but of the soul,” still applies. The appropriate implant must be decided preoperatively as must the best access route: periareolar, submammary, or axillary.
Surgical Repertory
Subglandular, prepectoral implant p. 115
Subpectoral implant p. 115
Three access routes: periareolar, submammary, and axillary p. 115
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


