19. Periorbital Rejuvenation with Autologous Fat
19.1 Introduction
The eyes are a central feature in facial beauty. Accordingly, the periorbital region and upper third of the face are areas of great interest and importance for the aesthetic surgeon. Not surprisingly, numerous chapters in this book discuss rejuvenation of these areas, including upper and lower blepharoplasty and browlift techniques. Although nonsurgical modalities, including neuromodulators (e.g., botulinum toxin) and fillers (e.g., hyaluronic acid), are frequently used as temporary approaches for facial rejuvenation in this area, they do not substitute for the long-term surgical options discussed elsewhere in this book.
When one of these surgical procedures is performed, injections of fat are an excellent option for fine-tuning and enhancing the final results. Adding volume to certain aesthetic subunits, particularly in the periorbita, is critical given the effect of aging on soft tissue volume and tone. In general, grafting autologous fat has become the filler of choice for many plastic surgeons and is considered superior to synthetic fillers for several reasons. 1 , 2 , 3 , 4 Fat is nearly an “ideal filler.” It is autologous, nontoxic, biocompatible, potentially removable, and easily available in most patients. 5 , 6 , 7 Additionally, with improved graft survival using newer harvesting and preparation techniques, the longevity of autologous fat can be greater than that of an injectable filler. In contrast to alloplastic implants, transplanted fat is more abundant, malleable, and resistant to infection. Because of the need for frequent reapplication of exogenous fillers, their cost may surpass that of fat injections.
For more than a decade, we have used autologous fat grafting for volumizing various facial subunits (e.g., upper lid sulcus), along with selective fine cannula aspiration for reduction of areas with senescent increases in fat deposits (e.g., perioral mound). 8 , 9 , Although each patient will present with unique anatomical variations, the periorbital region frequently needs volume redistribution with both removal of fat from some areas and addition of fat to others. This chapter focuses on the evaluation of patients undergoing periorbital procedures and the appropriate treatment with autologous fat grafting.
19.2 Periorbital Anatomy
Although a more detailed description of periorbital anatomy can be found elsewhere in this book, we focus on periorbital fat anatomy. The readers are also encouraged to review relevant orbital anatomy to understand more completely the pathophysiology of aging and surgical approaches. 11 , 12 , 13 , 14 , 15
19.3.1 Upper Lid
The most superficial layer of upper eyelid is composed of thin skin with orbicularis oculi lying just deep to it. There is little or no fat between the skin and the muscle layer. Deep to the orbicularis and cephalad to the tarsus is retro-orbicularis oculi fat (ROOF), a layer of fibroadipose tissue that is superficial to the orbital septum and above the superior orbital rim. As ROOF is thought to provide the smooth gliding of the orbicularis oculi muscle at the orbital rim, resection is not recommended. 16
The orbital septum is found deep to the orbicularis muscle and the ROOF. Superiorly, the septum is attached to the orbital rim, and inferiorly the septum blends into the levator palpebrae superioris aponeurosis approximately 1.5 to 2 cm above the lid margin. There are two distinct intraorbital fat compartments deep to the septum, the medial (nasal) and central compartments, which are separated by superior oblique muscle. The fat in the medial compartment is whiter and denser in consistency and contains a higher amount of adipose-derived stem cells. 17 In contrast, the fat in the central compartment is less dense and more yellow. Lateral to the central fat compartment lies the lacrimal gland, which is located in the lacrimal fossa on the posterior surface of the lateral superior orbital rim. A prolapsed lacrimal gland may appear as lateral upper lid bulging and may be mistakenly resected during upper blepharoplasty. 18 , 19
19.2.2 Lower Lid
As with the upper lid, the skin of the lower lid is thin, with orbicularis muscle just deep to it. Analogous to the ROOF on the upper lid, the suborbicularis oculi fat (SOOF) is located superficial to the orbital septum at the inferolateral aspect of the lower lid. Histologically, both ROOF and SOOF contain more fibrous tissue compared with orbital fat. 20
The lower orbital septum joins the capsulopalpebral fascia approximately 5 mm before inserting onto the lower edges of the inferior tarsal plate, which lies just deep to the orbicularis muscle. Unlike the upper lid, the lower lid has three intraorbital fat compartments: the medial (nasal), middle, and lateral compartments. The medial and middle fat compartments are separated by the inferior oblique muscle. During dissection for a blepharoplasty or an orbital floor surgery, great care must be exercised not to injure this muscle. The middle and lateral compartments are divided by the arcuate expansion of Lockwood’s ligament. The arcuate expansion combines with the inferior oblique muscle to form the capsulopalpebral fascia.
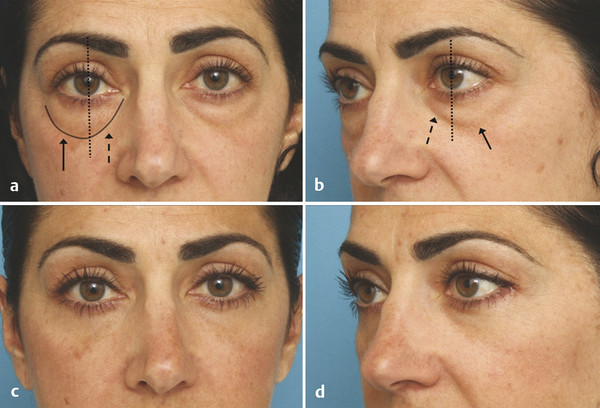
19.2.3 Orbitomalar Sulcus
The orbitomalar sulcus is an anatomical deformity comprising the tear trough (medially) and the lid–cheek junction (laterally) (Fig. 19.1). This deformity can be present even in young patients, but it often becomes more prominent with age. Patients with a prominent orbitomalar sulcus often complain of dark, baggy circles below their eyes.
This deformity results from dermal attachments of the orbicularis retaining ligaments (ORLs). The orbicularis oculi extends below the inferior orbital rim and inserts on the anterior surface of the superior maxilla through the ORLs. The ORLS are osseocutaneous structures that originate 5 mm inferior to the lower orbital rim, pass through the orbicularis muscle, and insert to the dermis. The ORLs are found circumferentially about the orbit, spanning from medial to lateral canthus tendon. 21 The ORLs divide the orbital compartment from the cheek compartment of the face. 22
19.3 Physiology of Aging
The effect of aging on facial skin and subcutaneous tissue is a complex process. Facial disharmony is the result of a complex interaction of the environment, changes in biomechanical properties of connective tissue, and differential soft tissue volume atrophy.
Excessive sun exposure accelerates the normal aging process. In contrast to the normal aging process, characterized by thinning of the dermis, actinically damaged skin is associated with thickened dermis. Microscopically, solar damage leads to elastin and collagen degradation in the dermis. Solar ultraviolet radiation leads to both direct and indirect skin changes by causing DNA damage and also leads to dysregulation of dermal connective tissues by altering the metalloproteinase mechanism.
Thinning of the aging dermis is associated with changes in the component of dermal connective tissue. Histologically, there is loss of total collagen content compared with the dermis from a younger individual. 23 The ratio of collagen type 1 to type 3 changes as well. Whereas the amount of type 3 collagen remains unchanged in aged skin, there is a decrease in type 1 collagen as a result of impaired collagen 1 synthesis. 24 The decrease in collagen content is thought to contribute to thinning of skin. In addition, because there is greater loss of collagen compared with elastic fibers, the aging skin loses its ability to resist deformation and becomes more elastic. An example of this phenomenon is upper and lower lid skin excess.
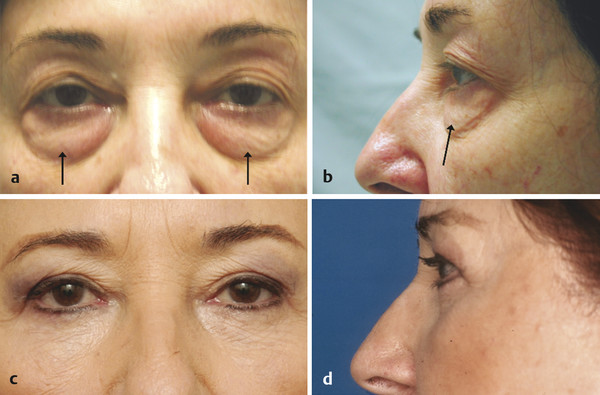
Another effect of collagen loss is seen with attenuation of fascia and laxity of retaining ligaments. Around the orbit, weakening of the orbital septum leads to fat volume displacement, clinically manifested by pseudoherniation of fat from the orbital compartments (Fig. 19.2). In the inferior lid, normal aging also produces volume deficiency that produces inferior orbital hollowing. With the descending of the malar fat pad inferiorly, along with the skin tethering to the underlying periosteum by the orbicularis retaining ligament, the classic V-shaped depression becomes apparent at the orbitomalar junction. The medial aspect of the depression is termed the nasojugal groove, and the lateral is called the orbitomalar groove. A youthful lower lid is short, characterized by concavity overlying the superior septal segment that transitions smoothly onto the convexity of the lower lid and cheek. 25 In contrast, in an aging lower lid, pseudohernia of orbital fat combines with malar fat displacement, producing the double-convexity deformity, separated by the orbitomalar groove. 26
Related posts:
 6. Facial Sculpting and Facial Slimming with Neurotoxins
6. Facial Sculpting and Facial Slimming with Neurotoxins
 22. Lower Eyelid Blepharoplasty
22. Lower Eyelid Blepharoplasty
 17. Secondary Facelifting
17. Secondary Facelifting
 5. Energy-Based Treatments for Facial Aging
5. Energy-Based Treatments for Facial Aging
 9. Male versus Female Facelift Surgery. Is There a Difference?
9. Male versus Female Facelift Surgery. Is There a Difference?
 12. Primary Superficial Musculoaponeurotic System (SMAS) Facelift and Neck Lift
12. Primary Superficial Musculoaponeurotic System (SMAS) Facelift and Neck Lift
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


