18 Facial Artery Musculomucosal Flap
Summary
The facial artery musculomucosal (FAMM) flap is a versatile locoregional pedicled flap that has gained popularity in reconstructive surgery. When tunneled into the nasal cavity, it provides plentiful vascularized tissue for larger septal perforation. Although technically challenging, it is associated with low morbidity and leaves no visible external scar.
18.1 Introduction
Over the past decades, regional pedicled flaps have increasingly been used to restore small- to medium-sized defects of the head and neck including nasal septum perforations. While small symptomatic perforations are traditionally closed by local mucosal flap, 1 , 2 the facial artery musculomucosal (FAMM) flap has become a popularized technique for the repair of large symptomatic septal defects (> 2–3 cm). 3 Other reconstructive options such as open rhinoplasty approaches, 4 , 5 , 6 , 7 , 8 , 9 , 10 , 11 , 12 nasal tissue expanders, 13 forearm free flap, 14 and pericranial flaps 15 have also been used for large septal deficits. Initially described in 1992 by Pribaz et al, 16 the FAMM flap is a relatively simple and timesaving procedure that avoids residual external scars of the face. 17
In this chapter, we describe and review an endonasal surgical approach using a pedicled flap, the superiorly based FAMM flap, as an alternative option for correction of large nasal septal perforation (NSP).
18.2 Indications
Large septal perforations (≥ 2 cm)
Septal perforation in patients with poor quality or lack of intranasal tissues such as those with previous radiation therapy in the concerned area, extensive ablative surgeries, or chronic cocaine abuse
18.3 Anatomy
18.3.1 Facial Artery Pedicle
The facial artery follows a cervical course after exiting the external carotid artery. It crosses the submandibular gland and reaches the inferior border of the mandible at the anterior limit of the masseter muscle. The facial artery travels in the cheek lateral to the buccinator muscle and the levator anguli oris, while remaining medial to the risorius, zygomaticus major, and the superficial layer of the orbicularis oris muscle. 18 , 19 The artery has a very tortuous trajectory on its way to the internal canthus to form the angular artery. Through this latter we can expect a retrograde flow from the ophthalmic artery, which originates from the internal carotid artery system. 20
The facial artery is located approximately 16 mm from the labial commissure. It sends off perforators of the jugal area and branches to give the superior labial artery among others. Several branching variations and terminal endings of the facial artery have previously been described. 21 The classification by Lohn et al includes 22 type I = angular, type II = lateral nasal, type III = alar, type IV = superior labial, type V = inferior labial, and type VI = undetected.
The facial vein usually runs posteriorly and in close proximity to the facial artery at the level of the mandible. It progressively diverges from the artery as it reaches the nose. Doppler flow studies have shown an average distance between the two vessels of 13.6 mm at the oral commissure and 16.3 mm under the alar base. 23 The vein begins at the internal canthus as the angular vein and runs along the nasogenian fold to become the facial vein.
18.3.2 Facial Artery Musculomucosal Flap
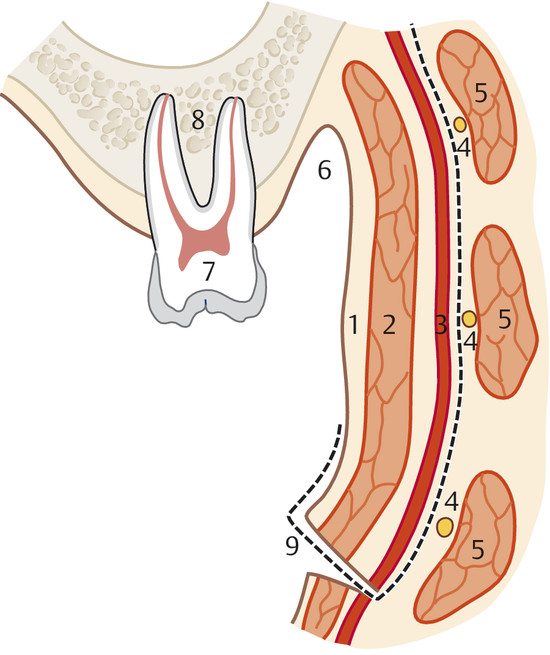
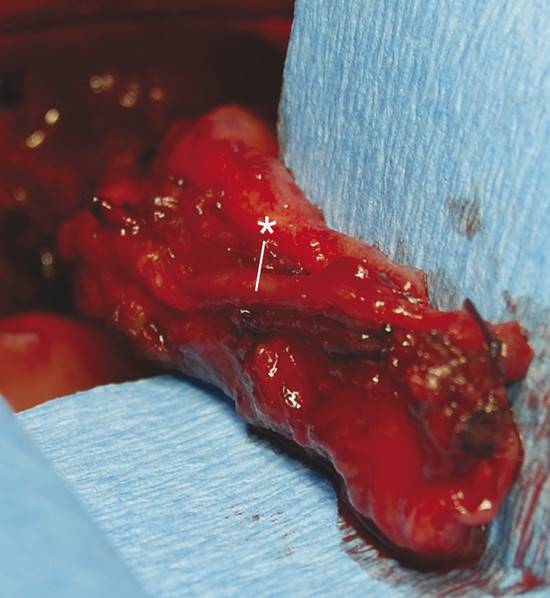
The FAMM flap is an intraoral cheek flap and includes the buccal mucosa, submucosa, buccinator muscle, and superficial layer of the orbicularis oris muscle (Fig. 18‑1). Superiorly based flaps are used for nasal septum perforations to maximize tissue length. Superiorly based FAMM flaps are pedicled on the angular artery and perfusion occurs through a retrograde flow. The facial artery is preserved on the entire length for the flap and kept attached to the buccinator muscle (Fig. 18‑2). The facial vein is usually not included in the flap as venous drainage is assured by a submucosal plexus. 24 The pivot point of flap is in the vicinity of the maxillary tuberosity or in the gingivolabial sulcus. The average width of the flap is 2.5 to 3 cm, and the pedicle base should be at least 1.5 cm to ensure adequate venous drainage. 17
18.4 Surgical Technique
The FAMM flap was first described by Pribaz et al in 1992 16 as a versatile musculomucosal flap harvested intraorally in the area of the jugal mucosa. It can be pedicled either inferiorly on the facial artery or superiorly on the angular artery. For the reconstruction of intranasal defects, a superiorly based pedicled FAMM flap will be harvested.
18.4.1 Anesthesia
Antimicrobial prophylaxis directed against oral cavity flora is recommended. After oral intubation, the endotracheal tube is positioned contralateral to the surgical bed. It can be held in place with transjugal or intraoral dental sutures. Neuromuscular-blockage will facilitate exposure of the oral cavity throughout the procedure. We do not recommend local infiltration of the flap outline with an epinephrine solution as it can provoke a spasm of the facial artery that may hinder its dissection.
18.4.2 Drawing the Flap
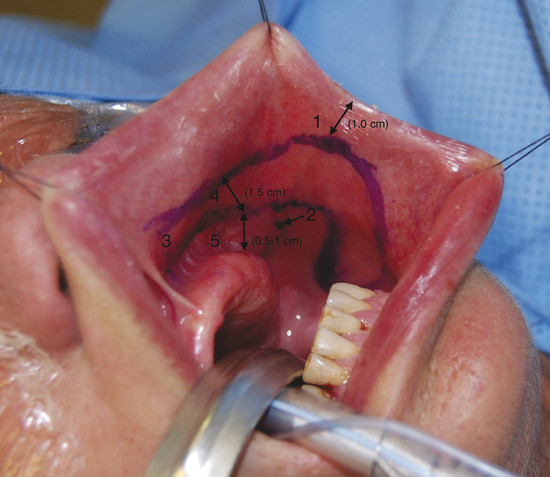
The buccal mucosa is exposed using two traction sutures in the upper and lower lips and a Weider’s tongue retractor (heart-shaped). Alternatively, Senn’s retractors or Gillies skink hooks can be used instead of traction sutures. With the anatomical landmarks in mind, an outline of the flap is drawn on the buccal mucosa (Table 18‑1). The anterior limit of the flap lays 1 cm posterior to the labial commissure to avoid its distortion after closure of the defect. The posterior limit of the flap lies just anterior to Stensen’s duct papillae. A distance of 0.5 to 1 cm is preserved between the posterior margin of the flap and the gingiva to facilitate wound closure (Fig. 18‑3). The use of a Doppler to identify the facial artery has been previously described 3 but will hardly ever modify the flap outline, as it relies on fixed anatomical landmarks. Moreover, the facial artery course outline is not reliable anymore after the mucosal incision because the mucosa becomes loose. Superiorly, the flap base is designed to hinge at the junction between the gingivolabial sulcus and first molar.
The distal end of the flap is designed according to the size and shape of the septal perforation. Measurement of the defect or usage of a template is mandatory and will allow an optimal flap outline. As the width of the FAMM flap is limited by the aforementioned landmarks (usually ~3 cm), the size and axis of the defect will decide whether the flap’s inset will be horizontal or vertical. For a long craniocaudal perforation, the flap’s inset will be horizontal, whereas a tall-vertical perforation will be covered with the flap inserted vertically.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


