18. Avoiding Complications in Facelifts
18.1 Introduction
Aesthetically, the face is the most privileged part of the body, and it directly relates to an individual’s identity; so the notion of elective surgical intervention to improve appearance may seem ludicrous to the casual observer. Reported complication rates after facelift surgery are actually quite low, however, according to a national survey representing more than 12,000 facelifts, which reported a major systemic complication rate of 0.1%. 1 To gain perspective, the annual risk of dying among licensed drivers in the United States, according to the National Highway Traffic Safety Administration, is about 1 in 16,000, which equals around 0.00625%. About 300 people die annually in commercial airline crashes of three billion passengers every year. That is around 1 in 10 million, or 0.00001%. 1 About 130,000 facelifts are performed annually in the United States, with one death occurring every 90,000 to 200,000 cases, 2 equaling about one to two facelift patient deaths per year, or 0.0008%. In other words, a facelift is safer than driving your car, but it is not as safe as flying commercially (Table 18.1).
Driving a car | 1/16,000 | 0.00625% |
Facelift surgery | 1/130,000 | 0.0008% |
Flying commercial airlines | 300/3,000,000,000 | 0.00001% |
This low risk does not mean the mortality risk in facelift surgery should be taken lightly. In 1994, two deaths occurred within 2 months at the prestigious Manhattan Eye, Ear, and Throat Hospital in New York City. The surgeons were distinguished international leaders in the field, and the patients did not appear to be high health risks, but it happened, totally astonishing plastic surgeons everywhere on the planet. 3
Plastic surgeons face risk themselves. In 1991 a woman in Bellevue, Washington, unhappy with her facelift, shot and killed the doctor who performed the surgery, and she later turned the gun on herself and committed suicide. 4 So facelift surgery can be very serious business! This chapter is about identifying complications associated with facelifts and helping the reader better understand risk management, thereby avoiding or minimizing the complications and maximizing the best possible result potential for each individual patient, thus shifting the risk–reward differential far in the reward’s direction.
Major risks can be categorized as systemic and regional. The systemic risks include potentially lethal conditions like deep venous thrombosis (DVT), venous thromboembolism (VTE), and pulmonary embolism (PE), as well as intraoperative anesthetic misadventures, postoperative medication abuse, cardiac events like myocardial infarction and cardiac arrhythmias, and respiratory disorders like obstructive sleep apnea (OSA), chronic obstructive pulmonary disease (COPD), and asthma. 5 Major regional risks can be broken down into vascular, neurological, wound healing, and traumatic surgical technique (Table 18.2).
Minor facelift complication risks are more localized to aesthetic problems, which can be devastating to the patient. They result from the surgery and include hairline and ear deformities, scar problems, abnormal contour changes, and distortions of facial shape and proportion. These topics are discussed in detail in this chapter. Psychological risk factors must also be carefully evaluated in the process of patient selection. 6
Avoiding complications begins and ends with the sound practice of good medicine. Graduating medical students take the Hippocratic oath, which sets the standard for medical professionalism and must be adhered to when performing surgery. Adherence to the oath engenders integrity and clarity of purpose and keeps the surgeon’s judgment sharp. Recommending for patients only surgical procedures that the surgeon would consider for loved ones or family members constitutes the proper contextual platform for surgery.
18.2 Patient Selection
A top-quality facelift is the result of a sophisticated process of planning and execution that begins with patient selection. The initial consult is a thorough exercise to gather information on many levels: subjective, objective, psychological, medical, family, work, social, and artistic. It includes an exchange of visual cues, verbal interaction, and a “hands-on” evaluation of facial tissue quality, volume, support, laxity, and mobility that allows the surgeon to identify specific diagnostic problems and to calculate the tissue shifts that would effectively correct the problems. The corrections are demonstrated to the patient while he or she holds a viewing mirror, and visualization of the anticipated result is discussed (Fig. 18.1).

The patient’s behavior and personality are subtly tested during this conversation, and inquiry into family situations, marital status, work, and personal interests may reveal anxiety, depression, or regressive tendencies that need formal psychiatric exploration before surgery is considered. 7 Careful drug history is important for patients on psychotropic medicines such as antidepressants and mood stabilizers because some drugs like venlafaxine hydrochloride (Effexor) can cause hypertensive problems with anesthesia. Under the guidance of the prescribing physician, patients taking Effexor often should be carefully switched to another antidepressant 6 to 8 weeks before surgery. Some patients are secretive and embarrassed about sharing psychiatric drug therapy, but positive, compassionate support from the surgeon will usually work wonders in getting patients to reveal personal issues. Drug and alcohol dependency issues need to be addressed appropriately, and referral for treatment initiated if necessary. Close communication with the patient’s primary care provider is crucial to avoiding complications from surgery, and a thorough physical with electrocardiography and laboratory testing is required for all patients over 40 years of age or for younger patients with a history of medical problems. The first and most foolproof way to avoid complications is to deny surgery to a high-risk patient. A caring, experienced staff is invaluable in recognizing “problem patients” and will most often alert the surgeon to potential dangers that he or she might miss. When dealing with the rare patient with sociopathic traits, it is often the nurse or patient coordinator who will “raise a red flag” about that person’s behavior. Such individuals can be elaborate storytellers, charming and delusional to the point that the doctor might not see it; but an expert staff will usually detect inconsistencies in their actions and alert the doctor about what they saw or felt. True sociopaths endanger all around them, and it is imperative never to perform elective cosmetic surgery on one. These patients must be managed in a firm, decisive manner. 8 Do not make promises that you cannot keep, and be proactive in referring to other qualified specialists. Recruit help if one of these cases arises to avoid a tragedy. 9
Excellent staff members are irreplaceable when dealing with a dissatisfied patient or one who has suffered complications; such staff members are competent, available, supportive, and reassuring when they are needed. Sometimes the surgeon might become frustrated when a patient keeps complaining about a problem and naturally may become angry, but the surgeon must never become angry. The doctor’s job is to manage problems and to help people, not to compound problems into complications. Maintaining professional objectivity and equanimity in demeanor will allow the surgeon to avoid almost all medicolegal complications. It is probably a good practice for the surgeon to not operate on patients who are really unlikeable, have no sense of humor, are plastic surgery “junkies,” cannot see the same problems the surgeon sees, impair the surgeon’s good judgment because of power and excessive influence, or are paranoid. Patients do not sue doctors they like. Recognize and discuss problems truthfully, and work to improve them. Although the goal is perfection, limitations are unavoidable. The idea is not to deny problems as though they are not there. It is to minimize their damage potential and their repercussions. Avoid operating on the following patients:
Patients you do not like
Those who have no sense of humor
Plastic surgery junkies
Patients who cannot see the same problems you see
Patients who have some power over you and can influence your sound medical judgment
Informed consent is essential to patient education and preparation for surgery. Specific forms should be available for each procedure, and they must include details explaining the procedure, the risks, and possible complications, as well as the goals for the surgery to achieve. The patient needs to read the information packet carefully along with a staff member and ask questions. If necessary, the patient talks to the doctor again to clarify all the issues. Having a friend or family member present for the consultation is often very helpful because this person might remember important information, the details of which overwhelm the patient. No guarantees are given. The patient initials each page and signs the signature page, attesting that he or she has an acceptable level of understanding about the operation. Finally, the witness, usually the staff member or other competent third party in attendance, signs the form. Photocopies are made for both the patient and the doctor’s files; by committing to surgery, the patient makes a leap of faith. Payment is collected during the preoperative appointment 3 weeks before surgery. Laboratory specimens are collected around 2 weeks before surgery, and medical clearance is required from the primary care provider or specialist such as cardiologist, pulmonologist, or psychiatrist before surgery can proceed.
Standardized photographs are essential and are taken either at the preoperative visit or the morning before surgery. Frontal, 45-degree oblique, profile, and profile-looking-down-at-the-floor views are taken. Animated photos showing platysma dynamics, forehead muscle action, or facial asymmetries are often taken as well, for intraoperative decision making and for comparing to the patient postoperatively. It is amazing to see how people forget what they looked like before surgery, and the set of pictures is a powerful tool to help manage an unhappy, picky, or obsessive patient after surgery.
18.3 Major Systemic Risks
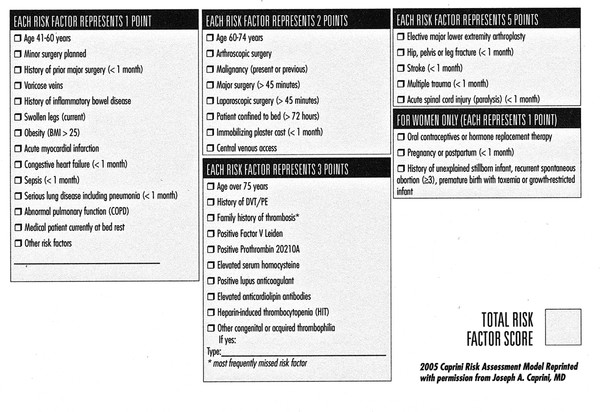
Potentially deadly risks need to be addressed and treated by medical specialists. DVT and PE rightfully receive much attention because they account for more than 50% of the deaths in outpatient surgery centers. 2 Yet the facelift patient data indicate that the occurrence rate of VTE events is quite low. In 2001, Reinisch did a retrospective study of 273 practices and found a DVT rate of 0.35% and a PE rate of 0.14%. 10 Nonetheless, because of the devastating potential of this complication, it behooves the surgeon to identify patients most likely at risk and try to eliminate this risk in the best possible way. A history of previous DVT, venous insufficiency, use of oral contraceptive or hormone replacement therapy in women, and long-distance travel, especially by airplane, should be noted and further evaluated. Pregnancy tests should be run on appropriate women. General anesthesia, obesity, and abdominoplasty surgery are associated with a greater risk of VTE. 11 The American Society of Plastic Surgeons VTE Task Force, as a valid method of assessing VTE risk, has endorsed the 2005 Caprini Risk Assessment Model. The American Society of Anesthesiologists (ASA) physical status (PS) classification has also been proven to be helpful in identifying patients at higher risk for VTE. (Fig. 18.2) 12
Controversy exists regarding the benefits versus the risks of preoperative chemoprophylaxis with low-molecular-weight heparin (LMWH) in facelift patients shown to be at higher risk for VTE as indicated by high Caprini scores (i.e., 8 or above). 13 Pannucci has demonstrated no significant increase in the occurrence of hematoma in general plastic and reconstructive surgery patients postoperatively when they are given perioperative LMWH 14 ; however, Durnig has shown that the risk of hematoma is significantly increased in facelift patients given perioperative prophylaxis. He had a 16% hematoma rate in patients given LMWH versus a 1% rate in those not given chemoprophylaxis. No patient in either group, 600 patients combined, suffered VTE, and the author attributed effective risk reduction to the practice of using intravenous sedation instead of general anesthesia and compression devices for the lower extremities. 15 Stuzin concurs and further advocates early ambulation. 16
In about two-thirds of cases, VTE events are asymptomatic, but within the first hour of a PE, the mortality rate is 10%. 17 Postthrombotic syndrome puts survivors at greater risk for subsequent VTE events. 12 Classic symptoms of PE are chest pain worsened by cough, shortness of breath, tachycardia, and hypotension leading to shock. The diagnosis of VTE events requires immediate hospitalization and intervention to dissolve the clots and restore vital cardiopulmonary function.
Obstructive sleep apnea creates problems in facelift surgery, including increased mortality risk. 2 OSA often manifests with the symptoms of snoring, frequent awakening during sleep with a choking sensation, and daytime somnolence. Patients suspected of having OSA should be referred to a specialist for in-depth evaluation before surgery is attempted. OSA poses obvious anesthetic airway risks, and ASA-PS guidelines are helpful in operative planning. Patients found to be at significant risk probably should not undergo surgery in a freestanding outpatient setting. 18 If an OSA patient is found to be a suitable candidate for facelift surgery, intravenous sedation, local anesthesia with regional nerve blocks, and the use of a laryngeal mask airway by a skilled anesthesia provider is effective and safe for airway control and patient comfort. Continuous positive air pressure (CPAP) devices can be very beneficial to patients suffering from OSA. Coordinating the use of a patient’s CPAP device after facelift surgery is somewhat difficult because the supporting straps are tight and can disrupt fine suture lines, but it can be done and is extremely helpful in maintaining normal blood oxygen levels. It is important that surgical and nursing staff be familiar with the equipment to best assist the patient. 11 Opioids and sedatives should be restricted because they can cause respiratory depression. These patients frequently have coughing fits, which increase bleeding risks; uncontrolled head movements; and inappropriate postoperative positioning during the recovery period. Therefore, best results in these patients can be compromised. These patients require careful monitoring, longer than most other patients, by attentive caregivers.
Cardiovascular conditions must be recognized and effectively controlled for successful facelift surgery to be achieved. Cardiac arrhythmias are a known mortality risk. 2 Patients with a history of a heart condition or an abnormal electrocardiogram must receive thorough evaluation and testing before clearance from their cardiologist. Close communication is crucial here to coordinate cardiac medication therapy and the timing of surgery. Oral medications can usually be taken with a small sip of water on the morning of surgery. Continuous intraoperative cardiac monitoring is essential, and contingency plans for administering intraoperative medications should be in place. Surgeons, anesthesia providers, surgical staff, and nursing staff should all be current and certified in advanced cardiac life support training, and hospital admitting privileges should be maintained by the operating surgeon. In the event of a significant acute cardiac event in surgery, the operating team should render appropriate treatment. Call 911! The facelift operative site should be controlled, and the wounds safely closed, and the patient transferred by ambulance and admitted to the hospital. Do not let ego get in the way of patient care in this situation. Call 911! It might save a life.
In uneventful cases of patients with cardiac conditions, continue postoperative monitoring overnight. Be certain the patient is discharged with a competent caregiver and attended by a responsible adult for the next week to 10 days. Prescribed medications must be carefully administered as directed because prescription drug mismanagement increases mortality risk in recovering facelift patients. 2 Do not neglect competent supervision of the patient during this important postoperative period.
Although patients over 60 years of age are at increased risk for cardiac and other complications, 19 there is not a significantly increased risk of complications in healthy older patients undergoing facelift surgery. 20 ASA physical status (ASA-PS) grades healthy patients over 70 years of age as ASA 2, and it is reasonable to assign an ASA status to each patient in assessing preoperative risk to be thorough in contemporary attempts to avoid complications in facelift surgery. Anesthesia staff cooperation in monitoring core temperature and actively warming patients to avoid hypothermia is important in all patients, but especially in older patients. Recognition of patients susceptible to malignant hyperthermia (MH) is crucial to avoiding this dreaded complication. Protocols need to be in place in the event of a case of MH, and dantrolene must be available for emergency use. Pulmonary conditions like COPD and asthma and metabolic conditions like diabetes should all be managed under the guidance of the patient’s medical specialist with the close rapport of the anesthesia provider. Perioperative medications must be carefully coordinated and administered to optimize patient care and are best managed by a certified, professional anesthesia provider.
Related posts:
 6. Facial Sculpting and Facial Slimming with Neurotoxins
6. Facial Sculpting and Facial Slimming with Neurotoxins
 22. Lower Eyelid Blepharoplasty
22. Lower Eyelid Blepharoplasty
 17. Secondary Facelifting
17. Secondary Facelifting
 5. Energy-Based Treatments for Facial Aging
5. Energy-Based Treatments for Facial Aging
 9. Male versus Female Facelift Surgery. Is There a Difference?
9. Male versus Female Facelift Surgery. Is There a Difference?
 12. Primary Superficial Musculoaponeurotic System (SMAS) Facelift and Neck Lift
12. Primary Superficial Musculoaponeurotic System (SMAS) Facelift and Neck Lift
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


