17. Secondary Facelifting
17.1 Introduction
The acceptance of cosmetic surgery by the baby-boomer generation has led to an increase in the volume of surgical procedures. Coupled with the rise in the number of procedures has been an increased life span in the same patient population. It is thus no surprise that patients who previously underwent a successful rhytidectomy are interested in further facial rejuvenation as they age. The American Society of Plastic Surgeons has estimated that 160,000 facelift procedures were performed in 2012, 1 representing a 6% increase in the number of procedures from the previous year.
Secondary facelifting has not received the attention that primary facelifting has received. 2 , 3 , 4 , 5 , 6 , 7 , 8 , 9 , 10 , 11 , 12 , 13 , 14 , 15 , 16 Most of the published series include few patients. In presented series, there are few patients for whom the surgeon performed both the primary and the secondary facelift. D Castro and Braga presented a series of 19 patients who underwent secondary facelifts. 4 The exact procedure performed for the primary operation was not noted, there was and no documentation as to whether any of the 19 patients had their primary procedure performed by one of the authors. Guyuron et al 5 presented a series of 33 patients who underwent secondary facelift procedures. The senior author performed both the primary and the secondary procedure in only three patients in the series. There was no documentation of the type of surgery performed at the primary procedure. Also, the technique used for the secondary procedure was not documented. They based their outcomes on survey data that were obtained mainly from patient recollection. The results from their series demonstrated that the average time from primary to secondary facelift was 8.48 years. Morales did not present any objective clinical data in his article, 6 but did present several clinical concepts regarding secondary facelifting. De la Torre et al. presented a series of 14 patients who underwent a reelevation of their malar fat pads. 9 In their series, the average time before the need for a secondary procedure was 40 months.
In an effort to evaluate the longevity of the result using a consistent facelift technique, we reviewed a series of 42 patients over an 8-year period in which the senior author performed both the primary and the secondary procedure. 17 The average length of time from performance of the primary procedure to that of the secondary procedure was 11.7 years. The reasons for early failure of the primary procedure, defined as a secondary procedure within 5 years of the primary procedure, were noted, as well as any associated complications. Nine patients required a secondary facelift before 5 years from the primary facelift (21.4%). The reasons for an early secondary facelift included loss of skin elasticity (five patients), an increase in subplatysmal fat and skin neck folds owing to weight gain (one patient), loss of elasticity secondary to protease inhibitors for human immunodeficiency virus (HIV) infection (one patient), loss of skin elasticity because of corticosteroid use (one patient), and residual fullness of digastric and residual submental fat (one patient).
17.2 Preoperative Facial Analysis
A careful preoperative analysis must be performed before performing a secondary facelift. The secondary facelift patient is definitely going to be older and is likely to have developed more medical problems since the initial surgery. Indeed, Guyuron et al 5 observed that 42% of patients planning to undergo secondary rhytidectomy had developed new medical issues, and 58% of patients had been started on a new medication since their initial facelift. As with the primary facelift, these patients need clearance from their primary care physicians before undertaking any secondary procedure.
It would be ideal to have copies of the operative reports from any previous procedures that had been performed, but it is frequently difficult to obtain copies of the operative reports because of the time interval that has passed between the primary and the secondary procedure. We continue to ask patients to bring in photographs of themselves at 5- to 10-year intervals in the past to appreciate their more youthful appearance and when they felt they looked their best.
We begin with a meticulous and comprehensive facial analysis. A careful notation is made of the scars from previous procedures. This analysis also includes a careful analysis of the hairline of the forehead, temples, and postauricular and occipital areas. Any distortions of the hairline are documented and are incorporated into the operative plan for the subsequent procedure.
The forehead and eyebrows are then examined. The distance from the eyebrows and orbital rim to the hairline is noted. The position of the eyebrows relative to the orbital rim is documented, and the amount of elevation required to restore the brow to an aesthetic configuration is noted at the medial brow, central brow, and lateral brow. The transverse forehead rhytids are then examined. Both the amount of transverse forehead rhytids and the relative strength of frontalis muscle contraction are evaluated to determine the amount of thinning that may be required of the frontalis muscle. The number of creases in the glabella resulting from corrugator superciliaris contraction is noted, as well as the number and depth of transverse creases at the nasofrontal angle from procerus muscle contraction. The depressor superciliaris is then tested by having the patient close his or her eyes tightly against upward resistance on the medial brow.
The upper eyelids are evaluated next. Many secondary facelift patients have previously had blepharoplasty procedures performed. The amount of excessive sagging skin is observed after the eyebrow has been placed into an aesthetically pleasing position. The amount of bulging fat in the medial and lateral aspects of the upper eyelid is noted. The level of the eyelid is documented for any possible eyelid ptosis. Typically, I have not performed blepharoplasty procedures at the time of browlift, facelift, and neck lifting. A previous blepharoplasty procedure with a large skin resection may result in an inadequate browlift for fear of creating lagophthalmos with the browlift.
The lower eyelids, face, and neck are then examined. Careful assessment is made of the amount of excess skin available for the procedure. The skin laxity found in secondary facelift patients is typically more vertical rather than the horizontal laxity seen in a primary facelift patient. The amount of excess skin is noted anterior to the tragus, anterior to the earlobe, and in the temporal region. An assessment is made of vertical excess skin in the cheek. The laxity of both the half of the neck and the whole neck is noted. The amount of skin available needs to be correlated with an assessment of the patient’s previous incisions and other needs with the secondary procedure (e.g., creating a preauricular hollow or creating hollowness in the submental area) for proper planning.
The lower eyelids are next evaluated. The position of the lateral canthus and the position of the lower eyelid relative to the iris are noted. The tone of the lower eyelid is tested using the snapback test. The bulging of the fat pads in the medial, middle, and lateral lower eyelid compartments is noted, as is a determination of the amount of excess skin. We have typically avoided lower eyelid blepharoplasty at the time of facelifting. A well-executed superficial musculoaponeurotic system (SMAS) facelift will improve the appearance of the lower eyelids by about 40%. Also, with the significant skin and subcutaneous tissue shifts that result from the facelift procedure, the surgeon may be tempted to remove too much lower eyelid skin, with the possibility of a postoperative ectropion.
The malar area and the crow’s-feet region are then evaluated. Many patients have fullness in the area below the infraorbital rim. This is localized edema and is not cured with the surgical procedure, nor do medications such as diuretics improve the situation. 18 It is important to explain this to the patient so that when the fluid and fullness recur after the procedure, the patient recognizes that this is not a failure of the procedure. The soft tissues fall off the malar eminences in both the primary and secondary facelift patient. This ptosis of the soft tissues falling to the fixed line of the nasolabial crease leads to fullness of the nasolabial fold and a deepening of the nasolabial crease. It also results in a skeletonization of the malar area, and when it is combined with the soft tissue ptosis in the region of the mandible, the result in the aging face is a boxy, angular configuration rather than the soft heart-shaped configuration of youth. Use of the SMAS to reposition the soft tissues of the face restores the softness over the malar areas and decreases the thickness of the nasolabial folds. 19 Traction on the SMAS does not deepen the nasolabial crease.
The presence and severity of crow’s feet are noted. Undermining over the orbicularis oculus muscle to the area of the lateral canthus and the lateral aspect of the lower eyelid gives a significant improvement in the appearance of the crow’s feet. A judgment should also be made regarding the depressor portion of the orbicularis oculus muscle, which we have termed the depressor orbicularis lateralis. When this muscle is strong, it will oppose any lifting of the lateral brow and result in recurrent ptosis of the lateral brow after a browlift procedure. The strength of the muscle contraction can be tested by having the patient smile and applying traction to the lateral brow. If the muscle action is strong, it can be divided to weaken the depressor action. 20 After the restraining communications between the orbicularis oculus and skin (crow’s feet) are released, 60% or more of the lower eyelid excessive skin is reduced by the shift of the facelift flaps. If the smile creases or connections are not released, there is no effect from the facelift on the lower lids. The release of the muscle–skin connections also changes the direction of the nasojugal groove from the oblique configuration of aging to the horizontal configuration of youth.
The perioral area is then reviewed. The patient is asked to smile to see whether the facial nerve is intact. This is especially important in the secondary facelift patient to document the status of the facial nerve preoperatively. The oral commissures are then evaluated to determine whether there is a dour and downturned appearance of the mouth. Use of the SMAS with adequate mobilization and precise vector placement of the main SMAS flap can elevate the corner of the mouth. 20 I prefer this approach to perioral rejuvenation rather than using excisional approaches such as those advocated by Weston et al. 21
The presence of fine vertical lines (smoker’s lines) of the upper lip is noted. My treatment of choice for these lines is dermabrasion at completion of the facelift procedure. Typically, the upper lip is treated at the time of the facelift. Dermabrasion usually results in improvement of the dark pigmentation of the lips and better color blending than other techniques. A biopsy of upper lip skin after dermabrasion will show much collagen buildup, which contributes to the smooth appearance. If circumferential perioral dermabrasion is needed, the lower lip and chin are done at a second stage sometime later. Performing circumferential perioral dermabrasion makes it difficult for the patient to open the mouth. Finally, an assessment of the patient’s lips is made, and if they are quite thin, the lips may be augmented.
An examination of the chin and neck is then performed. The laxity of the skin is noted. The neck is inspected for submental scars and their location. Frequently, these scars are actually placed into the submental crease, and they must be disregarded for the secondary procedure. The most inferior level of the skinfold is noted because the extent of the skin incision in the occipital area is perpendicular to this crease. The submandibular gland size and prominence are noted. The neck is examined for large digastric muscles that may create prominence in the submandibular area, as well as interfere with an aesthetic cervicomental angle and submental area. The presence of jowls and mandibular ligaments is noted. The presence of platysmal bands is noted, along with assessment as to whether the bands are tight and require transection of the platysma muscle. The positions of the cricoid cartilage and thyroid cartilage are noted. The neck is also inspected for any irregularities that may be present as a result of the primary surgery.
Finally, a careful evaluation of the ear is made. Sensation to the ear is tested to ensure that the great auricular nerve is intact. The angulation of the ear lobule from the axis of the ear is noted; it should normally be 10 to 15 degrees posterior to the ear axis. 22 , 23 Pixie ears are unfortunately seen in many secondary facelift patients, typically a result of excess skin removal and failing to place the ear in the appropriate position when tailoring the skin. To correct this deformity, an additional 4 to 5 mm of excessive skin is necessary anterior to the earlobe to allow the ear to transpose posteriorly at the time of the secondary procedure. It may not be possible to completely correct this deformity with the secondary facelift, and the patient should be counseled regarding this fact. The earlobes may be tailored with a wedge excision or trimming the caudal margin of the earlobe to make the earlobes harmonious with the facelift result. 24
17.3 Direction of Vectors of Aging
The vectors of the aging face are an inferior lateral and anterior displacement of the soft tissues. 25 The soft tissue changes are responsible for the characteristic appearance of the aging face, with deepening of the nasolabial crease, enlargement of the nasolabial folds, and the development of jowls. The soft tissues seem to fall off the malar eminence, creating the boxy and angular appearance to the aging face. The secondary facelift, however, has little skin laxity in the anteroposterior direction, and most of the skin laxity is found in a vertical direction. This direction of skin laxity sometimes makes it difficult to correct deformities that are the result of the primary surgery.
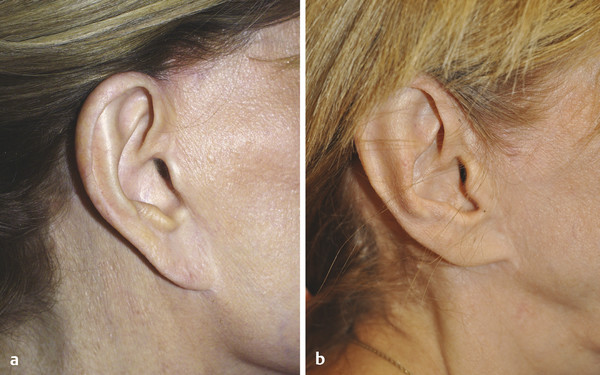
An example of this problem is seen in the case of the pixie ear deformity (Fig. 17.1). To correct this deformity adequately, about 5 to 15 mm of skin must be advanced posteriorly to transpose the earlobe posteriorly. If that same patient with a pixie ear also has fullness in the preauricular area, an additional 1 cm of skin may be required to make a concavity anterior to the tragus and correct the pixie ear. The timing for the surgery is very important because there may not be adequate skin laxity to correct deformities from the primary surgery. It is important to inform the patient of what can and cannot be corrected with the secondary surgery. If the patient’s understanding is limited, the limitations and possibilities should be documented in a letter to the patient.
Related posts:
 6. Facial Sculpting and Facial Slimming with Neurotoxins
6. Facial Sculpting and Facial Slimming with Neurotoxins
 20. Comparison of Midface Rejuvenation Techniques
20. Comparison of Midface Rejuvenation Techniques
 22. Lower Eyelid Blepharoplasty
22. Lower Eyelid Blepharoplasty
 5. Energy-Based Treatments for Facial Aging
5. Energy-Based Treatments for Facial Aging
 9. Male versus Female Facelift Surgery. Is There a Difference?
9. Male versus Female Facelift Surgery. Is There a Difference?
 12. Primary Superficial Musculoaponeurotic System (SMAS) Facelift and Neck Lift
12. Primary Superficial Musculoaponeurotic System (SMAS) Facelift and Neck Lift
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


