15 Bilateral Cross-Over Flap Technique
Summary
The correction of a septal perforation can be accomplished by various techniques. Despite the substantial available published literature on the treatment of septal perforations, the optimum technique is not fully established. The choice may depend on the etiology, size, and location, and also the surgeons’ preference, although there is a general perception that the size of perforation can be a significant factor for the success of the surgery, as surgical failures tend to occur more frequently in patients with large perforations. Bilateral coverage over the perforation with vascularized mucosal flaps seems also to be a contributor factor for complete closure, when compared to single unilateral flaps techniques. 1 , 2 The authors describe their technique, the so-called bilateral cross-over flap technique.
15.1 Indications
This surgical technique is conceived to repair medium-sized septal perforations, not larger than 2 cm in diameter.
This technique can be only accomplished if remaining cartilage covered with mucosa remains above the perforation.
15.2 Preoperative Considerations
Good visualization (0-degree endoscope) and use of very delicate surgical instruments ensure an easier, faster, and safer procedure. Adequate and delicate instruments are essential to shorten the surgical procedure. In some cases, otologic micro-instruments may be used.
Every initial step should be directed to prevent unnecessary mucosal trauma and bleeding keeping the edges of the perforation untouched. They will serve as pedicles for the flaps.
To facilitate tailoring and displacing the septal mucosa flaps, infiltration elevation can be accomplished initially by using a saline solution.
15.3 Instrumentation
0-degree scope
Scalpel
Suction elevator
15.4 Surgical Steps
The entire surgical procedure can be accomplished with a 0-degree endoscope. Choose the side with more space and more operating exposure. Keep the borders of the perforation untouched.
15.4.1 Step 1. Creation of Flaps
Superior Flap
After proper infiltration, begin by making a racket- or square-shaped incision (right side) beginning at the middle of the perforation anteriorly, extending up beneath the mucoperichondrium of the remaining cartilage superiorly, and making sure the size of the racket or the square delimited by the incision is enough to cover the perforation, and finish the incision at the middle posterior part of the perforation (Fig. 15‑1a, b).
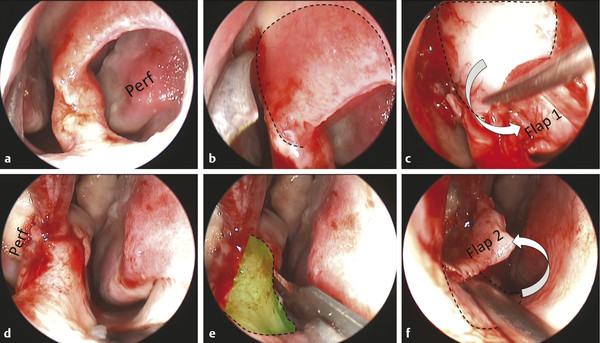
Elevate the mucoperichondrial flap carefully without injuring the mucosa that covers the superior half border of the perforation. This flap will cross over the perforation border to the contralateral nasal cavity (Fig. 15‑1c).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


