14 Unilateral Mucosal Advancement Flap
Summary
Unilateral advancement flap technique uses one side of mucosal flap from the bottom (inferior-based flap) and the top (superior-based flap) of the perforation of the nasal cavity. The contralateral side, uncovered with the flap, is healed by mucosal regeneration. In general, bilateral advancement flap seems the ideal method for reconstruction of the perforation. Even if mucosal flap of one side fails to close the perforation, contralateral mucosal flap could bring surgical success. However, a unilateral flap has the advantage of shortening of the operative time, and it can be used when the perforation is so large that the flap is hard to cover the perforation simultaneously on both sides. In the case of too large septal perforation, bilateral mucosal flap can cause an iatrogenic, new septal perforation at the site of flap elevation. Therefore, unilateral advancement flap is also a useful method for septal perforation closure.
14.1 Indications
Almost all of size and shape of septal perforations.
Patients do not have general inflammatory or vascular diseases.
The margin of septal perforation is not under the state of infection or inflammation.
14.2 Surgical Steps
14.2.1 General Aspects
Unilateral mucosal advancement flap technique uses two flaps, inferior- and superior-based flap, which are classified by their location in relation to the perforation (Fig. 14‑1, Fig. 14‑2). It is easier to develop large flaps from the inferior side of the perforation margin because more usable mucosa and space for handling instruments exist in the inferior nasal cavity. Therefore, the mainstay of the perforation closure is inferior-based flap. To facilitate sufficient mobilization of an inferior flap, incision is needed to be parallel to nasal cavity at the inferior aspect of the inferior turbinate. Dissection of the mucosa at nasal floor allows a maximal mobility of the flap. When more mobility of the inferior flap is required in spite of enough dissection at the inferior nasal cavity, the incision toward the anterior part of the flap, until it reaches the hemitransfixion incision, brings an additional mobility. The blood supply of the flap extended to hemitransfixion incision is provided only from the posterior nasal cavity, forming a monopedicled advancement flap. When the flap is getting larger, the risk of a new perforation increases. Especially, a simultaneous development of this flap on both sides has a possibility of a new perforation caused by the exposure of cartilage on the anteroinferior side of the septum on both sides. 1 , 2
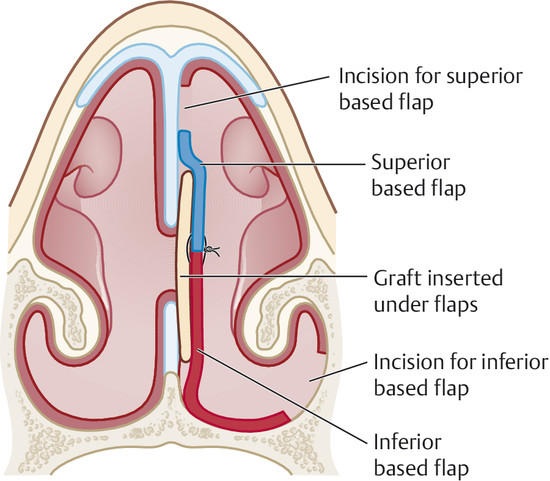
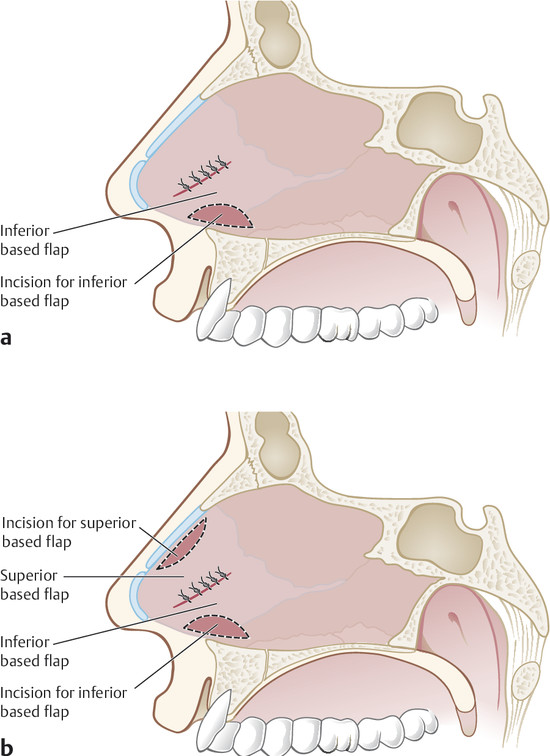
When the inferior flap cannot sufficiently cover the perforation or achieve a tension-free state at the closure site, a superior-based flap can be used. To harvest a large superior flap, the mucosal dissection is needed to be extended toward the mucoperichondrium at the undersurface of upper lateral cartilage. The mucosal dissection at the superior aspect can be more easily performed by using an open rhinoplasty approach. The simultaneous creation of bilateral superior based flap brings an interruption of the blood supply on the septal cartilage, and it can induce a new septal perforation. Therefore, a precise designing of flap size and location of incision are important factors for a successful closure of septal perforation.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


