14 The Evaluation and Management of the Cosmetic Patient
Abstract
“The Evaluation and Management of the Cosmetic Patient” addresses the treatment of patients seeking periocular and facial rejuvenation, who present many challenges. Inexperienced surgeons should approach such patients with great caution. The surgeon should be very adept at undertaking functional oculoplastic surgery before embarking on the exacting demands of cosmetic oculoplastic surgery. The surgeon should also have a good working knowledge of the myriad of nonsurgical approaches to the management of such patients, because surgery constitutes only one strategy for facial and periocular rejuvenation. Many patients who come to an oculoplastic surgeon typically seek rejuvenation or cosmetic options that provide good results, avoid typical stigmata of cosmetic surgery, and involve a minimally invasive approach, minimal risk, and minimal “downtime.”
14.1 Introduction
Patients seeking periocular and facial rejuvenation present many challenges, and inexperienced surgeons should approach such patients with great caution. The surgeon should be very adept at undertaking functional oculoplastic surgery before embarking on the exacting demands of cosmetic oculoplastic surgery. A good working knowledge of the myriad of nonsurgical approaches to the management of such patients should also be acquired to supplement or even replace surgical interventions where appropriate, because surgery only constitutes one strategy for facial and periocular rejuvenation. Many patients who are referred to or who present to an oculoplastic surgeon typically seek rejuvenation or cosmetic options, which provide good results while avoiding typical stigmata of cosmetic surgery but involve a minimally invasive approach, minimal risk, and minimal “downtime.”
14.2 Patient Consultation
14.2.1 Consultation Facility
A surgeon embarking on cosmetic surgery should evaluate his or her consulting facility setup and staff and ensure that these are tailored to the demands of cosmetic patients. This can be a major commitment. The initial contact made by a prospective patient may be with a receptionist, patient-care coordinator, secretary, office administrator, or a nurse. The surgeon should ensure that every member of staff is trained to respond to the initial contact in a professional and knowledgeable manner. The staff should aim to establish a rapport with the patient, which should be reinforced when the patient arrives for a consultation. The staff should be fully conversant with the range of surgical and nonsurgical treatments offered by the surgeon and by his or her nurse assistants and with his or her costs.
14.2.2 The Preconsultation
The preconsultation, preferably with an experienced aesthetics nurse practitioner, should begin with a detailed confidential health questionnaire that is very comprehensive and that requests detailed information about the following:
Previous facial cosmetic surgical and nonsurgical treatments, including botulinum toxin injections and dermal filler injections.
Past ophthalmic history including details of contact lens wear or previous refractive surgery.
Past dermatology history.
Past medical and surgical history including any tendency to excessive bruising or bleeding.
Drug and allergy history.
Social history including information about occupation, smoking, and alcohol consumption.
Family history including thyroid dysfunction or ophthalmic disorders.
It is extremely important, for example, that information about the prior use of periocular botulinum toxin injections is provided, because such injections can significantly affect the assessment and management of a patient with an eyebrow ptosis or blepharoptosis. The prior use of dermal filler injections with details of the fillers used and the location of the injections should be documented. Patients may present with a history of periocular or facial lumps of swelling that can be related to previous dermal filler injections. The questionnaire should be signed by the patient, declaring the information to be accurate. Ideally the patient will give permission for their family practitioner to be contacted.
The patient should be photographed from a variety of angles, with and without the use of a flash. Ideally, the photography should be standardized. Informed consent should be obtained for the use of the photographs. The precise purpose and intended use of the photographs should be explained to the patient.
A preconsultation with an aesthetics nurse practitioner is far less intimidating for the patient, and an initial rapport can be readily established that can be continued throughout the various phases of the patient’s care. The nurse can help to establish what the patient’s main concerns, goals, and expectations are and can discuss issues such as the timing of the use of postoperative makeup. The patient may reveal concerns about the outcome of treatments undertaken elsewhere, and the nurse can then prewarn the surgeon about these. The nurse can often identify a “difficult” patient and can express reservations about the patient to the surgeon. The patient is far more likely to divulge relevant information about the traumas of a recent separation, divorce, or bereavement, for example, to a nurse. These may prove to be major factors motivating the patient to seek cosmetic surgery for which they are psychologically ill-prepared.
Key Point
Patients should always be asked about the previous use of dermal filler injections.
14.2.3 The Surgeon Consultation
The preconsultation can save a lot of time, allowing the surgeon to concentrate on a comprehensive assessment and examination of the patient and time to counsel the patient about his or her concerns; the clinical examination findings; and the pros, cons, risks, and potential complications of the treatments discussed, as well as provide the patient with information about postoperative “downtime,” aftercare instructions, activity or driving restrictions, and time off work. The surgeon should allow sufficient time for the consultation and should encourage the patient to go home and consider the options presented with a minimum period of reflection of 2 weeks. The surgeon should follow up the consultation with a letter to the patient summarizing the following:
The patient’s complaints or concerns.
The patient’s past history.
The main clinical examination findings.
The management options discussed.
Preoperative recommendations, such as avoiding the use of aspirin or anti-inflammatory medications for 2 weeks before surgery.
The postoperative care requirements and the use of frequent drops or ointments, cool packs, and antibiotics.
The management of any postoperative pain.
The requirement to remain in the area of the clinic overnight for safety if the patient is travelling from a distance.
The expected duration of bruising and swelling and the anticipated time off work required.
The timing of postoperative clinic visits and the anticipated timing of the removal of sutures.
The risks and potential complications of surgery and the possible requirement for additional surgery or treatment.
A separate generic document that outlines all the risks and the potential complications of eyelid or facial cosmetic surgery, along with their management should they occur, should also be provided. It is always helpful to be able to direct the patient to the surgeon’s website, which should provide great detail about the procedures.
The patient’s letter should also be accompanied by a separate letter from the clinic administrator detailing all the costs of the treatment. Wherever possible, the patient should be encouraged to schedule another, shorter follow-up appointment to go over any outstanding issues and to sign a consent form. It can be difficult to remain focused in an initial consultation, and the patient can feel rather overloaded with information, particularly if the patient has not researched the subject in detail before the consultation.
The consent form should be typewritten and standardized and should never be completed on the day of surgery. It should contain a comprehensive list of all serious or frequently occurring risks, which should be explained in detail to the patient in a manner that neither frightens nor offends. The risks in the surgeon’s hands, not in the general medical literature, should be explained, providing the surgeon’s own experience of the procedure(s) to be undertaken. The surgeon should also make it clear how any potential complications would be managed and at what, if any, cost to the patient.
Key Point
A consent form for cosmetic surgery should never be completed on the day of surgery.
The dynamics of an effective cosmetic consultation are also very important. The surgeon should listen to the patient’s concerns without prematurely interjecting to provide an opinion. A patient who is nonspecific about his or her concerns and merely asks for recommendations should be encouraged to provide more detail so that the surgeon does not make inappropriate recommendations from having misunderstood the nature of the patient’s concerns. As a general rule, the surgeon should try to remain within the sphere of the patient’s complaint and not draw attention to other problems perceived by the surgeon, because this may cause offense. Constant interaction and adjustment of the discussion should occur to ensure that the conversation is progressing in line with the patient’s expectations. The surgeon can then determine how receptive the patient will be to alternative options that may not have been considered by the patient; for example, many patients who request an upper lid blepharoplasty are surprised to be told that they may benefit from a browlift.
Key Point
An astute patient will appreciate a surgeon whose clear objective is to provide good professional advice and recommendations that are in the best interests of the patient, rather than one whose main objective is to convert a clinic visit into a surgical case. Such a patient is far more likely to recommend the surgeon to others.
14.2.4 Patient Selection for Surgery
The selection of an appropriate patient for a particular surgical procedure is an acquired skill and is critical to success in cosmetic surgery. It is preferable to decline to operate on patients whose expectations are unrealistic, whose demands are unreasonable, or whose psychological preparedness is in doubt. It is also preferable to decline to operate on the patient who is unduly critical of previous surgery undertaken by a colleague but whose complaint is not legitimate. The surgeon should also beware of the manipulative or overfamiliar patient who is impolite to members of staff in the clinic but respectful toward the surgeon. The surgeon should always be aware of the possibility that a patient may have body dysmorphic syndrome, particularly where the patient’s concerns are out of proportion to the clinical examination findings (Box 14.1).
Box 14.1 The “Red Flag” Characteristics
Unrealistic expectations
Unreasonable demands
Cosmetic concerns out of proportion to clinical examination findings
Overfamiliarity with the surgeon
Overly and unreasonably critical of other colleagues
Inappropriate flattery toward the surgeon
Rudeness to clinic staff
Lengthy list of questions often derived from the internet
The patient has already decided on the surgical procedure(s) he or she requires
Impatience
Late for appointments but still expects full consultation time
Demand for surgery without respecting a period of reflection
The temptation to operate on or treat such a patient should be strongly resisted.
14.3 Nonsurgical Treatment Options
There are a wide variety of nonsurgical options to select from to help to achieve facial and periocular rejuvenation:
Botulinum toxin injections.
Dermal filler injections.
Intense pulsed light treatment.
Cutaneous laser resurfacing.
Chemical peels.
All nonsurgical treatments are associated with small risks of adverse reactions and unwanted side effects. The patient should be provided with detailed information about the treatments and the associated risks and potential complications. Informed consent should be obtained before undertaking any of these treatments. Oculoplastic surgeons who manage cosmetic patients should become expert in the use of botulinum toxin injections and dermal filler injections.
14.3.1 Botulinum Toxin Injections
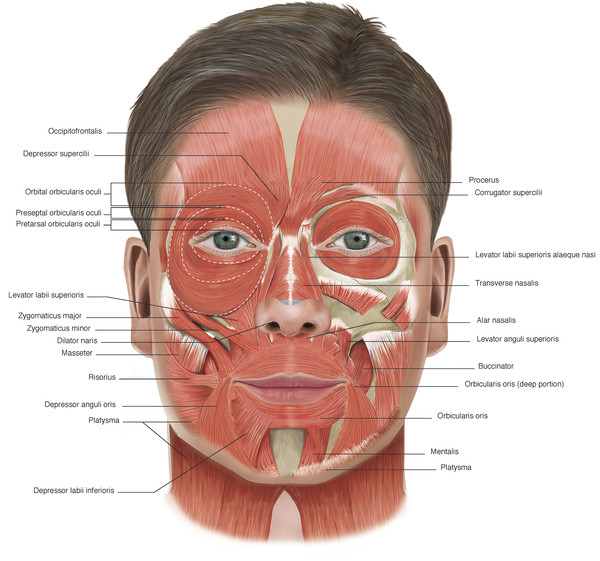
Botulinum toxin injections for periocular and facial rejuvenation can be used alone or in combination with other nonsurgical treatment modalities (e.g., dermal fillers) and can be used to improve the outcome of some surgical procedures. The injections have an excellent safety record, having long been used in ophthalmic practice for the treatment of essential blepharospasm and strabismus. Their safe and successful use in aesthetic treatments requires an understanding of the anatomy of the muscles of facial expression (Fig. 14‑1) and a meticulous injection technique, particularly in the periocular area. The major advantage of the use of botulinum toxin injections is the fact that any unwanted effects eventually wear off spontaneously, usually with no long-term sequelae.
It is always preferable to be conservative when treating a patient for the first time, because the effects cannot be actively reversed. It is preferable to offer the patient “top-up” injections after 10 to 14 days to achieve the best results. A clear record should be made of the site and number of injections given and the dose of each. Once the dose for that individual patient has been established, repeat injections are very simple to undertake, referring back to the previous treatment record.
I have used Dysport and Azzalure in my practice for more than 25 years. Dysport has a relatively long duration of action (approximately 4 months) and in my experience is very effective. Its onset of action is usually seen at approximately 3 days after injection, with the maximum effect seen approximately 7 to 10 days after injection. Other botulinum toxins are available for use (e.g., Botox, Xeomin, Myobloc), and the choice is a matter of surgeon preference.
Key Point
It is always preferable to be conservative when treating a patient for the first time, because the effects cannot be reversed. It is preferable to offer the patient “top-up” injections after 10 to 14 days to achieve the best results.
Procedure
A vial of Dysport contains a dry powder and is reconstituted by injecting 2.5 mL of sterile saline using a 3-mL syringe and a 21-gauge needle. The vial available in the United Kingdom contains 500 units of botulinum toxin. The vial and the saline should be checked carefully and the expiration date confirmed with an assistant. The solution in the vial is then withdrawn into a 1-mL Luer-Lock syringe using a 21-gauge needle. It is preferable not to withdraw more than 0.7 mL of Dysport into the syringe, because this makes it more difficult to control the injection. The needle is then removed and exchanged for a 30-gauge needle. Each 0.1 mL gradation on the syringe contains 20 units of Dysport, making it very easy to calculate the dose to be injected.
A vial of Azzalure is very similar but contains 125 units of botulinum toxin. The powder is reconstituted by injecting 0.63 mL of sterile saline using a 1-mL syringe and a 21-gauge needle. The needle is then removed and exchanged for a 30-gauge needle. Each 0.1 mL gradation on the syringe contains 20 units of Azzalure, also making it very easy to calculate the dose to be injected.
If the patient prefers, the areas to be injected can be prepared with a topical anesthetic gel to reduce the discomfort of injection. The patient should be advised to refrain from the use of aspirin or anti-inflammatory agents for 10 to 14 days before injection to minimize the risk of bruising. Bruising increases the risk of diffusion of the toxin to unwanted areas. The patient is instructed to keep his or her arms by the side during the injections. The practitioner should wear gloves. The injections are given perpendicular to the skin and directly into the underlying muscle (Video 14.1). For the glabella it is useful to ask the patient to frown maximally during the injections to actively contract and bunch up the brow depressor muscles. The injections should be given quickly, and immediate firm pressure should be applied to the injection sites for 2 to 3 minutes to avoid bruising. The patient should avoid vigorous exercise for a few days after the injections. The patient should be prepared to return for further adjustment injections if required after a period of approximately 10 to 14 days.
The injections can be given at a number of different sites:
The glabella.
The lateral canthi.
The sides of the upper nose.
The forehead.
The lower eyelid.
The chin.
The jawline.
The neck.
The upper lip.
The superior aspect of the nasolabial folds.
The Glabella
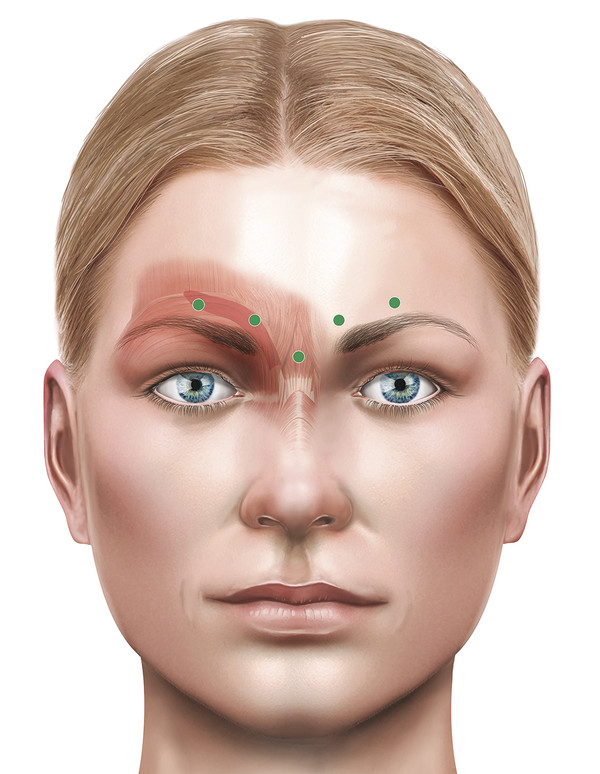
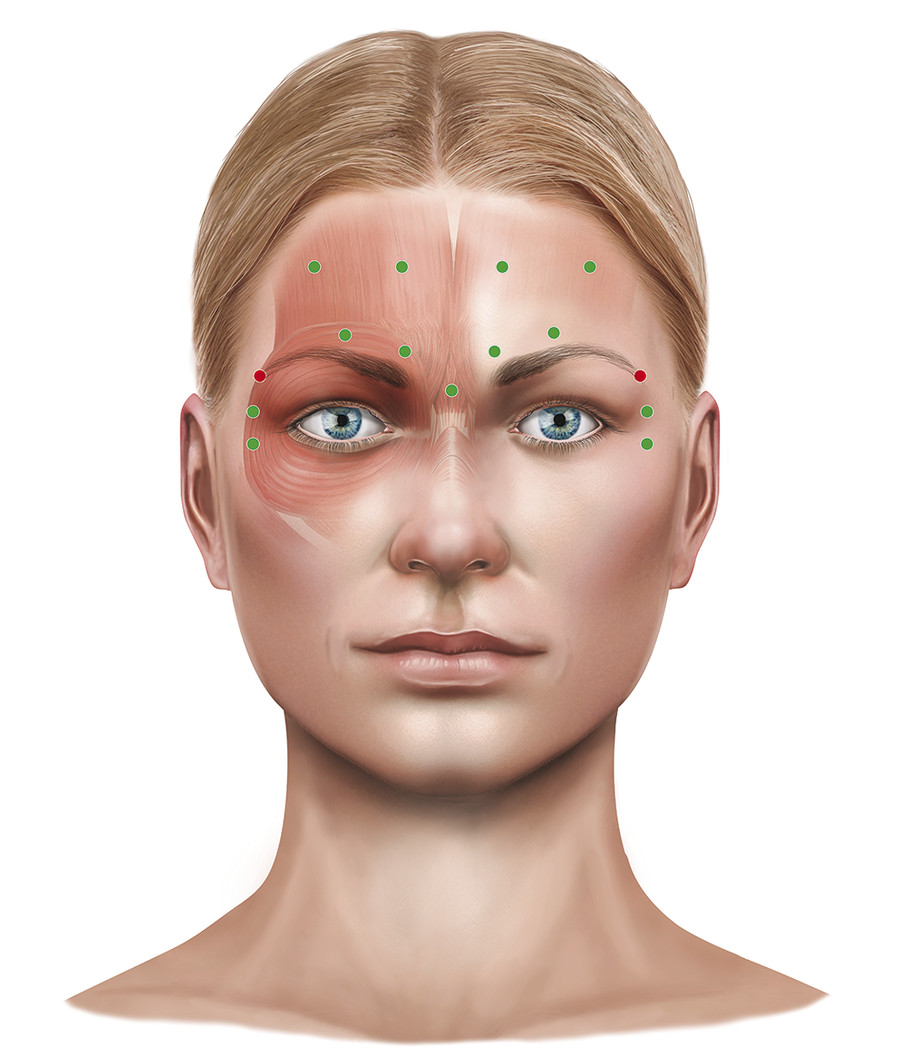
The most common site for injection is the glabella, targeting the corrugator and depressor supercilii muscles and the procerus muscle. This softens or removes glabellar frown lines and a horizontal line at the root of the nose. Lines that persist despite paralysis of these muscles require the use of dermal filler or fat injections. The injections are typically given as four to five separate injections with a total dose of 70 to 120 units of Azzalure. The patient is asked to frown to establish the degree of muscle contraction, and then the injections are given quickly into the muscles, injecting at 90 degrees to the surface of the skin, moving from the right to the left side, with a right-handed surgeon standing to the right side of the patient. Care should be taken not to extend the injections to include the adjacent frontalis muscle unless this is intended. Extension to involve the medial or central aspects of the frontalis muscle will result in a typical temporal peaking of the brows, particularly on attempted raising of the brows. This is a tell-tale sign of poorly administered botulinum toxin injections. It is commonly referred to as a “Mephisto effect.”
A typical treatment record for a patient is shown in Fig. 14‑2.
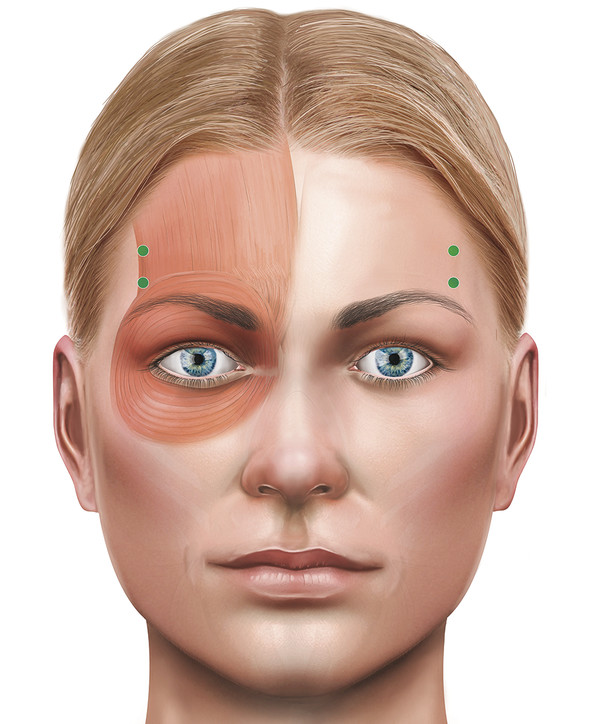
Should temporal peaking occur, it can be addressed with injections given into the lateral frontalis muscle fibers. A typical treatment record for a patient is shown in Fig. 14‑3.
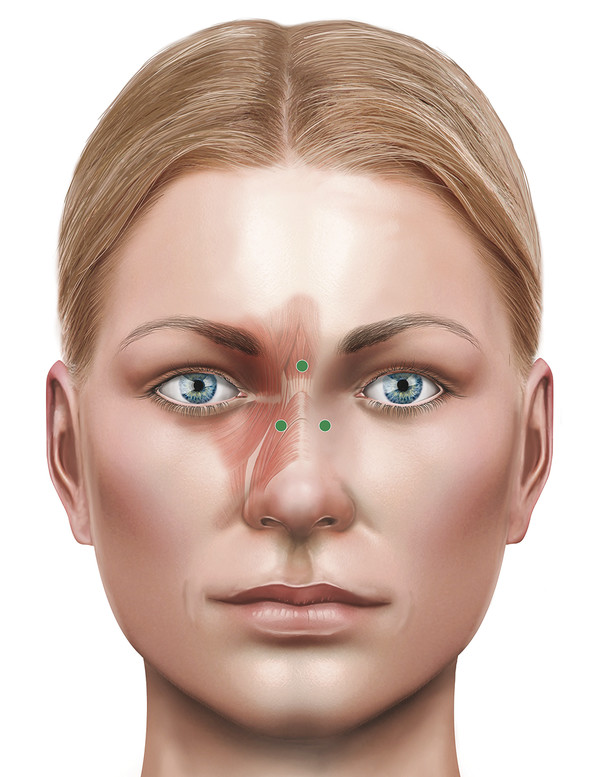
For horizontal lines at the root of the nose, the injections should target the procerus muscle. Some patients develop “bunny lines” when smiling from overaction of the nasalis muscles. These can be easily treated. This typically requires a single injection on each side of the nose, each containing 5 to 10 units of Azzalure (Fig. 14‑4).
Patients treated with injections of botulinum toxin given into the glabella who also experience migraines often notice a significant improvement in their migraines.
The Lateral Canthus
The muscle that is targeted at the lateral canthus is the orbicularis oculi muscle. A series of three to four to five injections are given after asking the patient to forcibly close the eyes and then relax. The visible veins at the tail of the brow are carefully avoided. The total dose used varies from 30 to 60 units. This treatment softens or removes lateral canthal rhytids. It can also effect a mild to moderate browlift, particularly when used in conjunction with glabellar injections, because of the unopposed action of the frontalis muscle (Fig. 14‑5a,b). If more of a browlift is also desired, an additional injection is given at the tail of the eyebrow temporally. The dose and injection sites can be modified to take into account any preexisting brow asymmetry.

A typical treatment record for a patient is shown in Fig. 14‑5c.
The Forehead
Great care should be exercised when injecting into the forehead. The muscle that is targeted in the forehead is the frontalis muscle. The frontalis muscle is much weaker than the brow depressor muscles and usually requires a much lower total dose to achieve the desired results. The treatment softens horizontal forehead lines very successfully, but an overtreatment can also result in a very unsatisfactory bilateral brow ptosis, particularly in patients who already have low brows. The patient should be counseled about this possibility and, again, an undercorrection should be the initial aim of treatment. Typically, a series of 4 to 12 injections, each at a dose of 3 to 5 units, are given across the forehead after asking the patient to raise the eyebrows. The dose and location of each injection may be amended, taking into account the visible muscle action, the extent and depth of horizontal forehead lines, and any asymmetries of the brows (Fig. 14‑6).
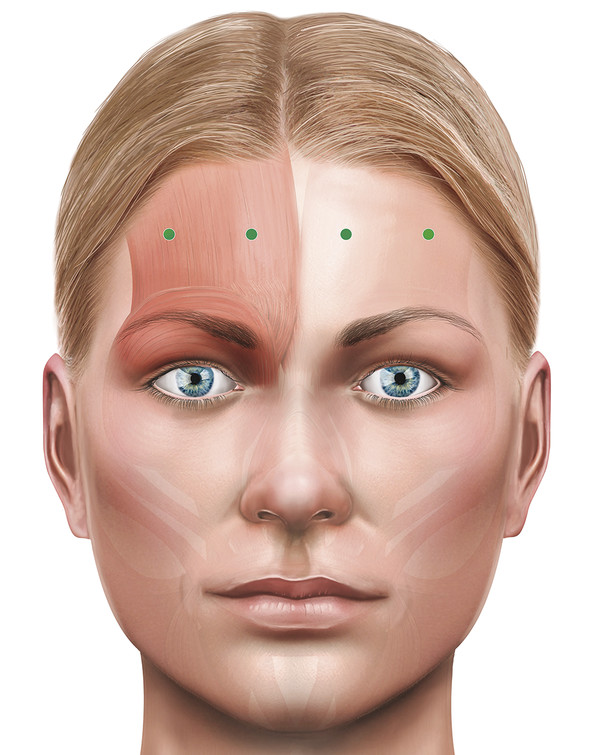
A typical treatment record for a patient is shown in Fig. 14‑7.
The Lower Eyelid
Injections in the lower eyelid should be confined to the lateral half to lateral third of the eyelid and should be very conservative. The muscle that is targeted in the lower eyelid is the preseptal orbicularis oculi muscle. The medial aspect of the lower eyelid is avoided to prevent any risk of spread of the toxin to the inferior oblique muscle, which could result in diplopia. Typically two to three injections are given at a total dose of 3 to 6 units. Higher doses can result in a retraction of the lower eyelid or the appearance of a malar “bag” in a predisposed individual related to loss of support of the lateral cheek by the weakened orbicularis muscle.
A typical treatment record for a patient is shown in Fig. 14‑8.

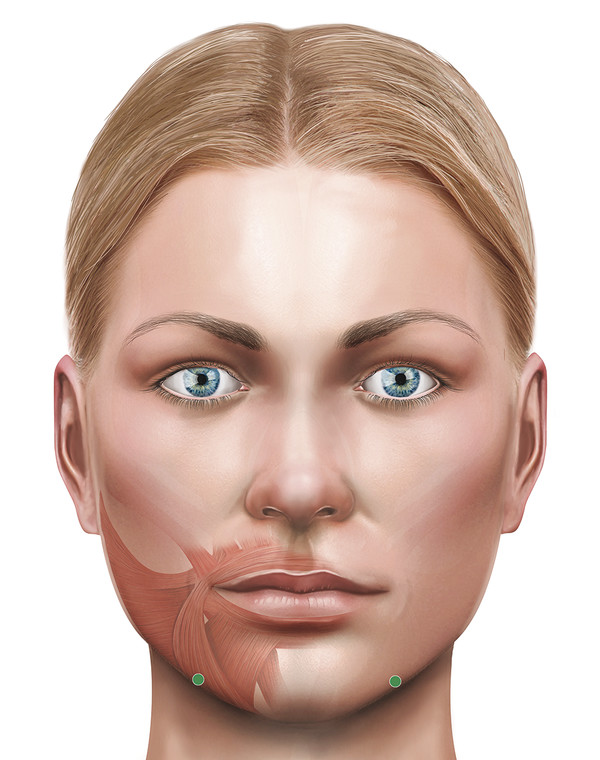
The Chin
Injections into the chin can help to improve a horizontal line or dimpling of the skin in this area. The mentalis muscle is the target muscle. Typically, two separate injections are given at a total dose of 10 to 15 units. Injections given more laterally over the mandible target the depressor anguli oris, which can help to lift the outer aspect of the lips, raising the smile. Typically, a single injection is given into each muscle at a dose of 10 units. A conservative approach should be adopted to avoid any problems with speech, eating, or drinking because of the involvement of the depressor labii inferioris.
A typical treatment record for a patient is shown in Fig. 14‑9.
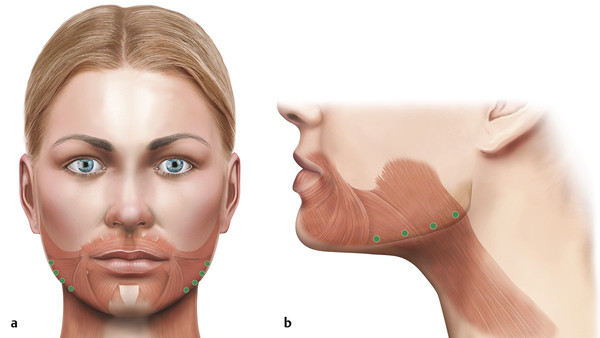
The Jawline
Injections along the jawline can help to improve the appearance of early jowling. The platysma is the target muscle. Typically 3 to 4 injections each of 5 to 10 units are given along the jawline.
A typical treatment record for a patient is shown in Fig. 14‑10.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


