12 Pharyngeal Flap Surgery
Introduction
The pharyngeal flap is the most widely used surgical treatment for restoring velopharyngeal competence. Tissue from the posterior pharyngeal wall is attached to the soft palate, creating a permanent static obturation of the nasopharynx with two lateral ports left for nasal airflow. Ideally, these ports remain patent during respiration and the production of nasal consonants and close during the production of oral consonants.
Pharyngoplasties designed to correct hypernasal speech secondary to velopharyngeal insufficiency (VPI) date back to the latter half of 19th century. In 1876, Schoenborn1 in Germany documented the first true inferiorly based pharyngeal flap surgery. This operation entailed suturing a flap of tissue from the posterior pharyngeal wall into the velum, with the pedicle of the flap inferiorly based. A decade later, Schoenborn2 modified his approach, creating the pharyngeal flap with the pedicle superior in the pharynx so as to maximize soft palate movement. In 1930, Padgett3 popularized the pharyngeal flap in the United States by documenting the use of a superiorly based flap for patients with cleft palate in whom primary surgical repair had been unsuccessful in producing normal resonance during speech. By the 1950s, the pharyngeal flap had become widely adopted for the correction of VPI. With the contributions of Hogan and Shrprintzen in the 1970s, surgical success rates continued to rise. Hogan4 (1973) introduced the concept of lateral port control, whereas Shrprintzen et al.5 (1979) advocated tailormade flaps. Collectively, these surgical advances resulted in the operation becoming the mainstay of contemporary velopharyngeal surgery.
Surgical Indications
Whether large or small, central gaps in the velopharyngeal sphincter mechanism found on videonasalendoscopy are the most amenable to correction with a pharyngeal flap ( Fig 12.1 ). To affect velopharyngeal closure, the side walls of the velopharynx must buttress against the inset flap. Lack of lateral wall movement prior to flap placement is not essential, as movement often develops over time through a course of postoperative speech therapy.
Preoperative Considerations
Surgeons must be vigilant regarding possible sources of airway obstruction. Identifying such sources prior to surgery minimizes the possibility of causing postoperative obstructive sleep apnea. Patients with adenotonsillar hypertrophy may require an adenotonsillectomy prior to the placement of a pharyngeal flap. A 6-week interval should elapse between procedures. Alternatively, an intracapsular tonsillectomy can be performed at the time of the pharyngeal flap procedure.
Patients with a history of retrognathia should be assessed for the adequacy of their upper airway and screened for sleep apnea. Airway concerns in these patients often warrant overnight polysomnography, which provides information that is helpful in determining the appropriate timing for surgical intervention. Performing a pharyngeal flap on a young child with retrognathia may severely obstruct the upper airway, necessitating a flap takedown, continuous positive airway pressure, or a tracheotomy. By contrast, allowing a retrognathic child additional time for growth often allows a flap to be performed without the complication of airway obstruction. Although superior speech outcomes are generally associated with surgical intervention at younger ages, a delayed approach is advisable in these patients.
There is a high incidence of velocardiofacial syndrome (22q11.2 chromosome deletion) in patients with VPI. These patients may also have medialized internal carotid arteries that could complicate a planned surgical procedure. Medialized vessels can be visualized on flexible endoscopy, and adjustment to a planned procedure can be made. Magnetic resonance imaging of the neck is not generally required in these patients.
Preparing for Surgery
Prior to surgery, the recording of the preoperative nasopharyngoscopy exam is reviewed to determine the level, pattern of closure, lateral wall motion, and the plane of attempted velopharyngeal closure (see Fig. 11.15). Anatomic landmarks are identified on the video that can be used to locate this level in the patient.
Surgical Procedure
A Dingman mouth gag is inserted and the patient is placed into suspension.
The posterior pharyngeal wall is visualized and palpated to identify any significant vessels in the operative field. In patients with velocardiofacial syndrome, the internal carotid arteries may be medialized.
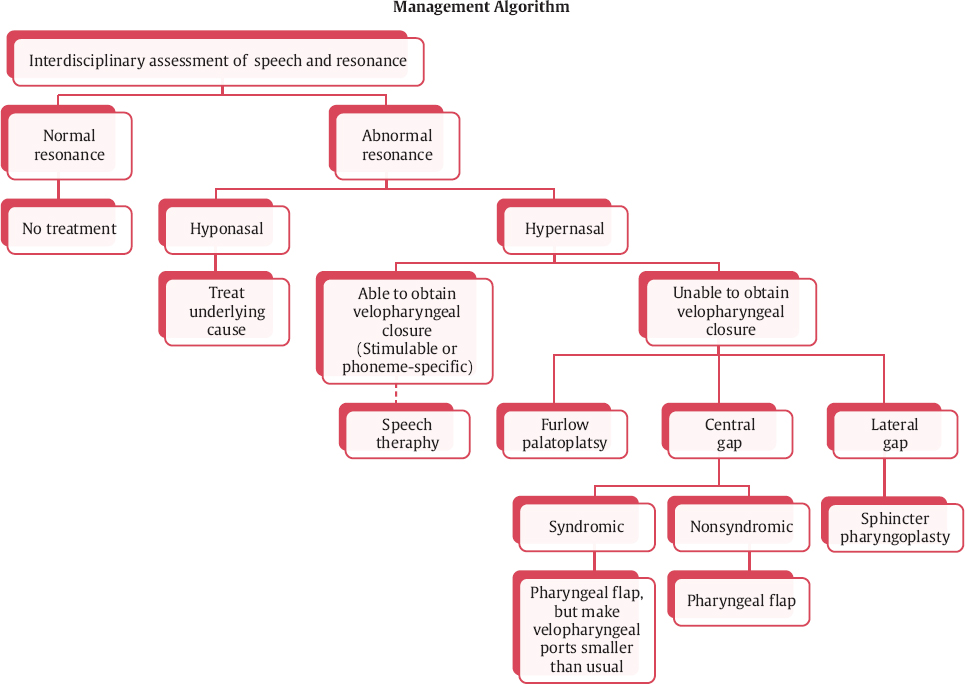
Fig. 12.1 Algorithm for treating velopharyngeal insufficiency. Furlow double-opposing Z-plasty palatoplasty is an option for small gap or touch closure with midline bubbling, which is not discussed in this chapter.
These vessels are deep to the prevertebral fascia and do not interfere with the operation; however, increased care must be taken in raising the flap.
Proposed posterior pharyngeal wall incision lines are infiltrated with 1% lidocaine with 1:100,000 units of epinephrine to induce vasoconstriction and ease the raising of the flap. The posterior aspect of the soft palate is similarly infiltrated at the level of velopharyngeal closure. This will be 5 mm cephalad from the free edge of the soft palate in children. Care should be taken to avoid distorting the tissues with the injection.
The standard flap width generally runs from a point approximating the posterior tonsillar pillars ( Fig. 12.2 ). The inferior extent of the flap should be near the midpoint of the tonsil. The length of the flap can be checked by estimating the distance from the posterior pharyngeal wall to the free margin of the soft palate, and then measuring down from the level of velopharyngeal closure. Care should be taken not to elevate a flap that is too long, as it may adhere to the posterior pharyngeal wall in a position below the level of velopharyngeal closure.
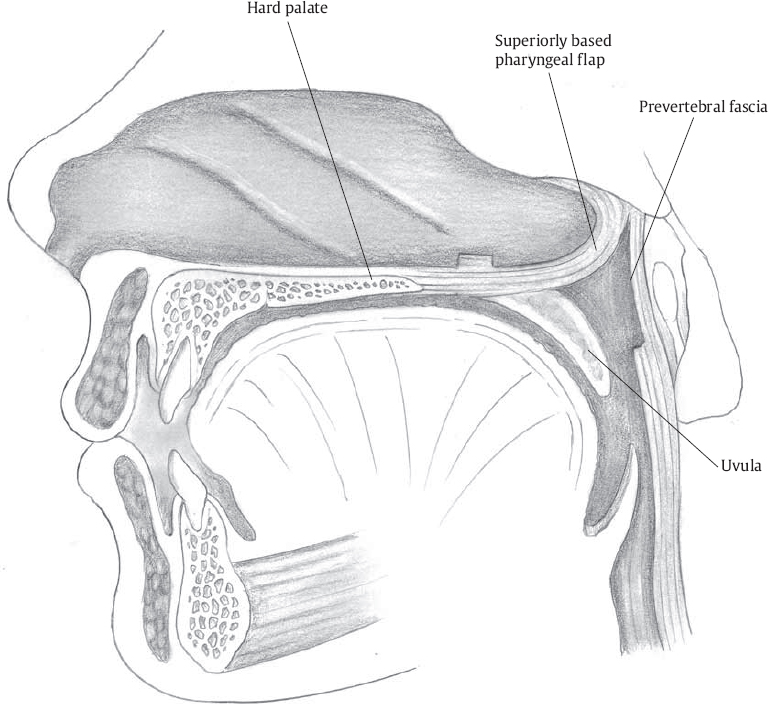
The superiorly based pharyngeal flap is elevated by incising down to the prevertebral fascia. This fascial layer is bright white in color, and the plane will be essentially avascular. It can generally be elevated bluntly after the inferior incision is completed. The flap should be elevated high into the nasopharynx. Hemostasis can be accomplished with monopolar cautery.
The lateral limbs of the superiorly based flap incisions are curved slightly laterally near the base of the flap to assist with creation of the lateral ports, and to ensure as broad a vascular pedicle as possible.
Flap elevation needs to be high into the nasopharynx, to the natural level of velopharyngeal closure. Failure to raise the flap high enough will result in an inferior tethering of the free edge of the soft palate, further compromising velopharyngeal function. If the flap is low, it will not be positioned to allow for proper velopharyngeal closure.
The inferior two-thirds of the donor site is closed with 3-0 Vicryl suture (Ethicon, Somerville, NJ). Undermining of the surrounding mucosa is rarely necessary. Suturing the mucosa directly to the prevertebral fascia prevents tenting of the mucosa and the creation of dead space. Superiorly, the donor site is left to granulate. Overzealous closure of the donor site superiorly can lead to nasopharyngeal stenosis.
A pocket is created on the posterior aspect of the soft palate. The incision must be at the level of velopharyngeal closure. The central aspect of the incision is made with a right angle Beaver blade. The palate is everted anteriorly with forceps. The incision is made into the soft palate. Care must be taken not to extend the incision inferiorly along the tonsillar pillars. The lateral aspect of the incision is made with palate scissors, again everting the palate for adequate visualization. One tine of the scissors is placed within the previously created pocket in the midline, and the tine is slid laterally along the plane of velopharyngeal closure. The scissor is turned such that the blades are perpendicular to the plane of the soft palate.
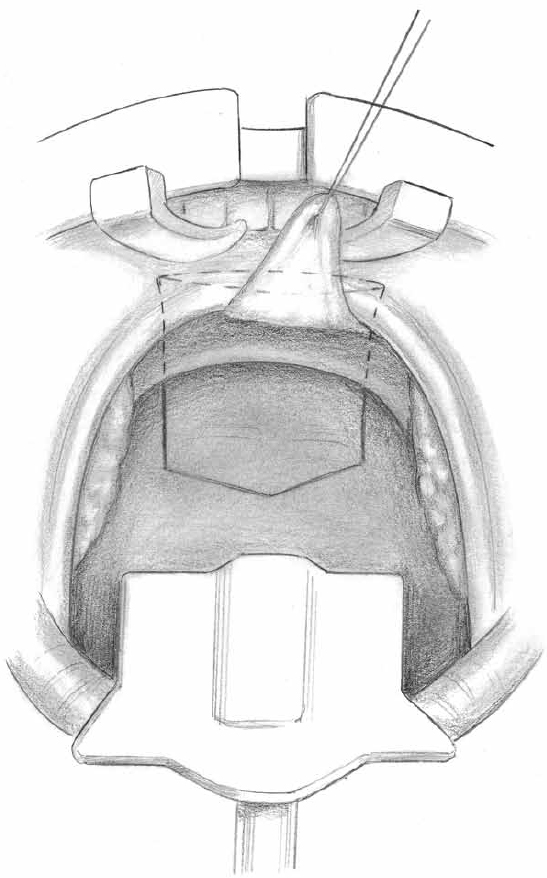
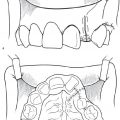
Fig. 12.2 Designing the flap. Uvula is retracted superiorly, the apex of the flap is a chevron shape and its inferior most point is at the midtonsil, and its width is the majority of the posterior pharyngeal wall (tonsillar pillar to tonsillar pillar).
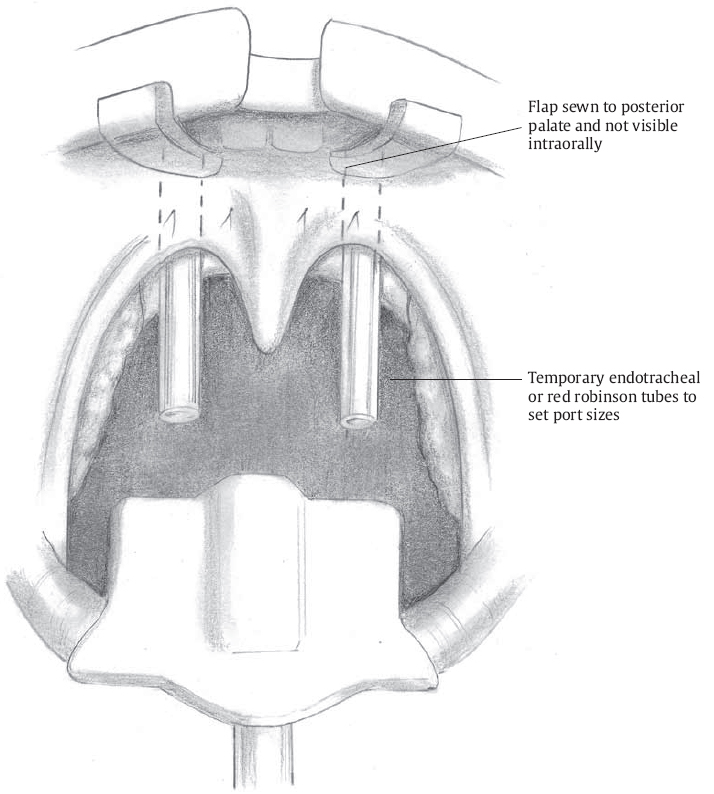
Nasal stents are placed transnasally into the hypopharynx. These stents are used to size the lateral ports; 3.5 mm endotracheal tubes are used for children age 6 and younger, whereas 4.0 mm endotracheal tubes are used for children age 8 and older. For children 6 to 8 years of age, endotracheal tube stent size is determined by the size and weight of the child. The stents define the final size of the lateral ports.
Starting with the lateral sutures, the pharyngeal flap is positioned into the soft palate. A 3.0 Vicryl suture is placed laterally, going through the oral surface of the soft palate and exiting the previously created fishmouth incision in the soft palate.
The suture is placed in the pharyngeal flap at the junction of the proximal and middle thirds of the flap. The suture is placed in the muscle and submucosa only; the squamous mucosa is not included in this suture.
The suture is then passed through the fishmouth incision of the soft palate and exits into the oral cavity within 2 mm of its initial pass, completing the horizontal mattress suture.
The suture is pulled (not tied) to position the flap into the palate. A mirror is used to check the size of the lateral port created when the flap is inset into the soft palate. The flap should touch the endotracheal tube, leaving space anterior and posterior to the endotracheal tube stent ( Fig. 12.3 ). The flap should not wrap tightly around the stent, as nasopharyngeal obstruction will likely develop. The suture is loosened, and the opposite lateral suture is placed in similar fashion and checked.
Two paramedian sutures are similarly placed to finish the insetting of the flap.
The sutures are tied, starting with the lateral sutures. Care must be taken to approximate the flap into the pocket without strangulating the tissue. Care also must be taken to ensure that the free end of the flap is positioned such that the muscle of the flap is in contact with the raw surface of the soft palate. The squamous mucosa of the flap cannot reside within the soft palate pocket.
A final check of the position of the flap and size of the ports is undertaken ( Fig. 12.4 ). The flap should not be visible from the oral cavity, as it needs to be high in the nasopharynx.
The endotracheal tube stents are positioned in the oropharynx, with the tips at the level of the mid-tonsil.
The endotracheal tubes are secured to the upper lip with tape and trimmed.
A number 6-8 French suction catheter is measured to direct the suctioning of the stents postoperatively. The catheter should extend 5 mm beyond the tip of the stent to ensure continued patency of the tube.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


