12 Lateral Nasal Wall Flap
Summary
Recently, a novel technique based on the use of pedicle lateral nasal wall (PLNW) flaps, either anterior (APLNW) or posterior (PPLNW), has proven to be a reliable and versatile reconstructive option for extensive defects of the skull base. Based on the later evidence, a PLNW flap may serve as an alternative procedure to reconstruct large nasal septum defects. The lateral nasal wall receives blood supply from a multiple anterior, posterior, and superior arterial branches, although its main arterial trunk arises posteriorly from the posterior lateral nasal artery (a branch of the sphenopalatine artery). The lateral alar artery (branch of the facial artery) and anterior ethmoidal artery supply the anterior and superior areas of the APLNW flap. These blood supplies may allow an anteriorly or posteriorly PLNW flap design to close septal perforations.
12.1 Indications
Medium (1–2 cm) and/or large (> 2 cm) size nasal septal perforations
Nasal septal perforation without osteocartilaginous support
Rescue flap for nasal septal reperforation
12.2 Contraindications
History of cauterization or embolization of sphenopalatine artery
History of cauterization of anterior ethmoidal artery
History of dacryocystorhinostomy on the ipsilateral side of the flap
12.3 Anatomy
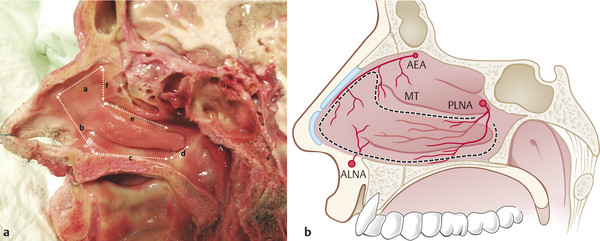
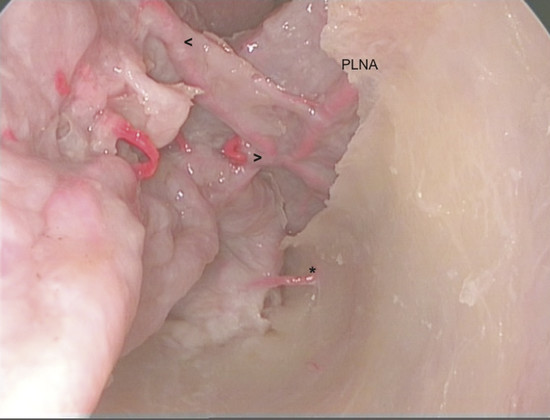
Understanding the vascular anatomy of the lateral nasal wall is crucial for harvesting the PLNW. 1 , 2 The useful area of mucosa of the PLNW (Fig. 12‑1a, b) covers superiorly from the axilla of the middle turbinate, then goes inferiorly up to the piriform aperture until the floor of the nose, and inferiorly it goes to the posterior insertion of the inferior turbinate. Finally, a superior sagittal plane limits it extension at the level of the lateral wall of the maxillary sinus till the perpendicular plate of the palatine bone where the posterolateral nasal artery (PLNA) is found. Depending on the defect, one can use anteriorly or posteriorly based flaps. The anteriorly based flaps will receive most of its blood supply from the anterior ethmoidal artery branch of the ophthalmic artery and anterior-lateral nasal artery (ALNA) branch of the facial artery. Posteriorly based flap are based on the branches of the sphenopalatine artery, mainly from the PLNA (Fig. 12‑2). In the mucosa of the lateral nasal wall, the PLNA runs anteroinferiorly over the perpendicular plate of the palatine bone and gives branches to the middle and inferior turbinates and fontanelle. Lee et al 3 studied 50 cadaveric specimens and observed that the PLNA ran downward on the perpendicular plate of the palatine bone and then coursed a little posterior to the posterior wall of the maxillary sinus in 42% and anterior to the posterior wall in 18%. Wu et al 4 studied the vascular anatomy of the PLNA in 11 cadavers. They observed that the PLNA mean outer diameter is 1.10 ± 0.11 (range: 0.82–1.30) mm and enters the inferior turbinate on the superior aspect of its lateral attachment, 1 to 1.5 cm from its posterior tip, and divides in 2.50 ± 0.52 (range: 2–3) arteries as part of inferior turbinate circulation.
Regarding the anatomy of the flap, Alobid et al 5 conducted a study on 40 de-identified computed tomographic (CT) angiographies and 20 hemicranial cadaver specimens to correlate the area and length of the PLNW flap with the nasal septum in order to plan surgery for septal perforation. On CT angiographies they demonstrated an average PLNW flap area of 10.80 ± 1.13 cm2, with a septal area (22.54 ± 21.32 cm2) that was significantly larger than the total PLNW flap area (14.59 ± 1.21 cm2). The average length of the flap was 5.58 ± 0.39 cm, whereas the septum was 6.66 ± 0.42 cm; therefore, the PLNW flap is insufficient to reconstruct the entire septum. On the cadaver study, they showed that the length of the PLNW flap was 5.28 ± 0.40 cm. These results demonstrate that measurements obtained from CT scans are reliable data and similar to those found in the radiologic study, and one can repair at least 80% defect with a PLNW flap. Regarding anteriorly based flap for septal perforation, there is no evidence available, and even though it is feasible, the managing of the flap itself is difficult and it has a limited range of movement.
12.4 Surgical Steps
12.4.1 Sinonasal Cavity Preparation
Cottonoids impregnated with a solution of 1:10,000 epinephrine are placed in the nasal cavity bilaterally during the surgical setup. At the beginning of surgery, the sites corresponding to the planned incisions are injected with lidocaine 1% with epinephrine 1:100,000. One must avoid injecting the area adjacent to the flap’s vascular pedicle (i.e., it causes vasospasm of the pedicle potentially impairing its viability) and the inferior turbinate (i.e., it may be equivalent to an intravascular injection).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


