10 Cleft Rhinoplasty
Introduction
Clefts of the lip, alveolus, and palate are the most common congenital facial malformation. Clefts of the lip and alveolus occur with typical nasal deformities that can range from subtle to profound changes in the aesthetics and function of the nose. Correction of the cleft nasal deformity is complex and often is addressed in stages. Although the importance of primary cleft rhinoplasty performed at the time of primary lip repair is clearly recognized, many cleft patients require secondary or “definitive” cleft lip rhinoplasty later in life. The fundamental anatomic corrections of the cleft lip nasal deformity include repositioning of the cleft-side lower lateral cartilage (LLC), alignment of the caudal septum, creation of dome symmetry, elongation of the columella as needed, correction of alar webbing, medialization of the cleft alar base, and providing structural support.1 These corrections, in turn, must also bring relief of subjective nasal obstruction.
Part of the difficulty of cleft rhinoplasty is the need to adapt to the variety of techniques used in previous cleft procedures, the great variety of anatomic aberrancy in cleft deformity, and the variable effects of prior surgical scarring. Selection of the optimal secondary rhinoplasty technique for a given patient requires deciphering the kinds of previous interventions and evaluating the residual deformities at present. No single technique addresses all of the deformities of the typical secondary cleft lip nasal deformity.2 Therefore, this chapter describes the more widely used techniques and makes recommendations on which ones to use for the menu of anatomic deformities found in the cleft nose.
Anatomic Considerations
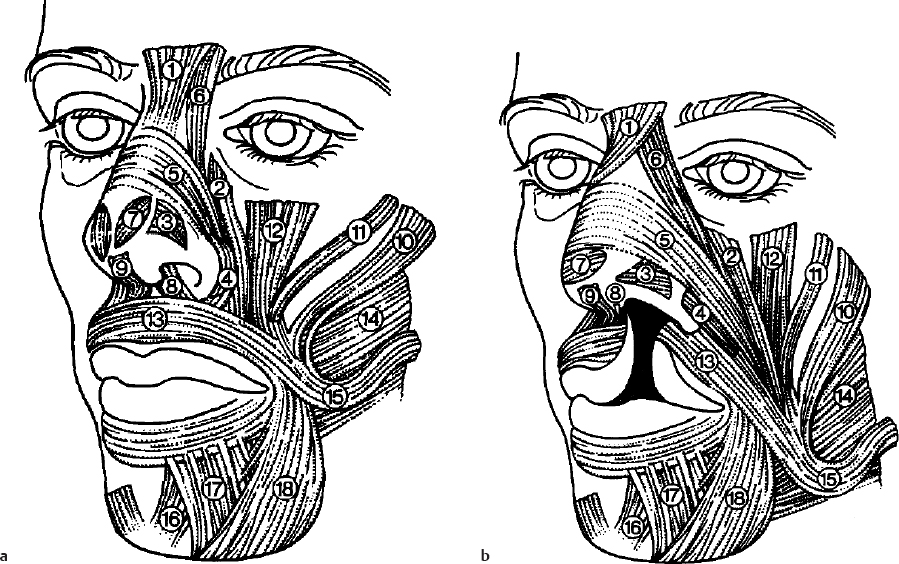
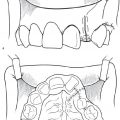
The nasal problems seen in the mature cleft nasal deformity are a combination of original, developmental, and postoperative factors.3 The original nasal deformity in the patient with unilateral cleft can largely be attributed to one or a combination of factors: aberrant facial musculature, hypoplasia of the skeletal (maxillary) base, and asymmetry of the skeletal framework.4 Anastassov, Joos, and Zollner catalogued in great detail the primary muscle dysmorphism and the influence of the aberrant muscle insertions on creating the cleft nasal deformity ( Fig. 10.1 ).5 Although the inferoposterior pull of the orbicularis oris muscle on the cleft-side alar base is well known, there are other nasal muscles with aberrant developmental vectors of pull that contribute to the final cleft nasal deformity moves. During contracture of the procerus muscle, nasal asymmetry from the middle vault is accentuated by the lateral motion from attachments to the contralateral upper lateral cartilage (ULC). The levator labii superioris alaeque nasi muscle is oriented more horizontal, inserting more inferiorly and laterally. This depresses the LLCs against the ULC, thus narrowing the internal nasal valve. This abnormal orientation of muscle pull also serves to lengthen the ala. The larger transversus nasalis muscle, which runs deep to the LLC but on top of the ULC, is torqued inferomedially on the cleft side contributing to the hanging ala. The dilatator nares posterior muscle is malpositioned more horizontally and behind the alar groove on the cleft side. During contracture of this muscle, the LLC and alar base are displaced more inferiorly. Lastly, the aberrant depressor septi nasi muscle inserts on the noncleft side together with its counterpart muscle to asymmetrically (toward the cleft side) contract the columella and nasal tip inferiorly.
Typical unilateral cleft lip repairs medialize the cleft-side alar rim and base, which results in tension on the already malpositioned LLC and buckling. In addition, inferior displacement of the lateral side cleft lip during primary repair comes at the expense of lateral vestibular lining, causing stenosis over time.6 The final position of the alar base changes with growth, but potentially can be too medial or too lateral. Hypoplastic nasal tissue, impaired growth, and surgical scarring contribute to asymmetric growth and dysmorphism.7 The most common secondary cleft nasal deformities are as follows8:
Retrodisplacement and underprojection of dome on the cleft side
Foreshortened columella on the cleft side
Lateral slumping of the medial crus of the LLC
Alar hood formed by the LLC and alar rim
Alar-columellar web
Insufficiency of vestibular skin at the vestibular dome
Varying nostril orientation
Malpositioned alar base
Deficient nasal floor
Caudal septal deflection to the noncleft side
Timing of Repair
Primary cleft rhinoplasty at the time of lip repair can have valuable and lasting influence on the resultant nasal anatomy and structure. Many, including these authors, support the role of primary rhinoplasty in guiding future growth of the lower third of the nose.9–11 Some patients who undergo primary cleft rhinoplasty have minimal nasal asymmetry and no functional compromise at the completion of nasal growth by adolescence and skeletal maturity. Although controversy exists regarding the impact on nasal growth, one longitudinal study by McComb and Coghlan12 found no significant disruption of nasal and midfacial growth lasting into adulthood. Ridgeway et al.13 presented cephalometric data following caudal septal repositioning during primary cleft rhinoplasty that resulted in lasting improvement in septal deviation and contralateral turbinate hypertrophy. A detailed discussion of primary cleft rhinoplasty is outlined in Chapters 4, 5, and 6 of this book.
Despite the benefits of primary cleft rhinoplasty, the majority of patients with cleft are still left with some anatomic deformity and nasal obstruction. In some cases, these problems are so severe that intervention is warranted prior to the completion of nasal growth. As outlined by Shih and Sykes, an “intermediate” cleft rhinoplasty can have a role in two distinct clinical scenarios: (1) the presence of significant nasal obstruction contributing to obstructive sleep apnea, and (2) children suffering severe psychosocial distress from facial disfigurement.14 The intervention is kept conservative and focuses on repositioning of the caudal septum with inferior turbinate reduction as needed. There are two time points when intermediate cleft rhinoplasty is recommended, depending on the specific problems of each patient.15 The first window of opportunity is between 4 and 6 years of age: this predates the typical onset of self-awareness and psychosocial impact of peer opinion, and may coincide with lip revision surgery if needed. The second window is between 8 and 12 years of age after completion of all orthodontic and alveolar bone grafting. A long-standing principle of nasal surgery is to have a stable platform on which to build. Low-level evidence suggests that repositioning the caudal septum and alar base is more effective if the skeletal maxillary architecture is anatomically normalized.
For the majority of cleft patients, however, there is a sound argument to delay definite rhinoplasty until after completion of nasal growth. This conservative approach has long been adopted for standard pediatric rhinoplasty protocols. Advocates of waiting until facial maturity cite the potential effects on nasal/midfacial growth of septoplasty and nasal osteotomies. This delays definitive rhinoplasty to ages 14 to 16 years for females and 16 to 18 years for males. For the subset of patients with cleft with significant malocclusion, orthognathic surgery is completed after skeletal maturity, and thus would precede any definitive rhinoplasty. If Le Fort I maxillary advancement is prior to completion of mandibular growth, revision orthognathic procedures would be necessary, further altering the nasal position.16 See Table 10.1 for a recommended timeline for secondary cleft rhinoplasty care.
Techniques
Nasal Base and Maxillary Augmentation
The underlying skeletal support of the nose is ideally addressed prior to definite rhinoplasty with alveolar bone grafting; however, simultaneously premaxillary grafts are also feasible. Careful assessment of the skeletal base architecture can determine if alveolar bone grafting and/or LeFort I (maxillary) advancement are needed prior to definitive cleft rhinoplasty.17,18 These skeletal procedures increase the projection and support of the lower third of the nose without significant alteration of the position of the nasal dorsum. Modest augmentation of the premaxilla with onlay grafts can be performed at the time of definitive cleft rhinoplasty, but the bony foundation of the maxilla should ideally be established.19–2 1 The anterior nasal spine is often deviated to the noncleft side and hypertrophic at the time of adult repair. The correction includes repositioning of caudal portion of the septum, osteotomy or rongeur of the hypertrophic nasal spine, and excision of the septospinal ligament. A columellar strut is typically indicated for multiple reasons, including maintaining tip support after trimming of the congenitally curved portion of the caudal septum.
Nasal Dorsum
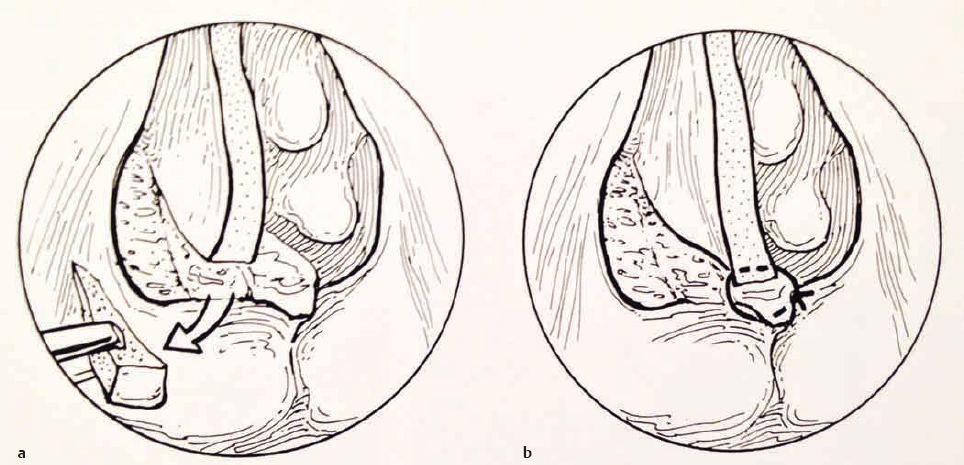
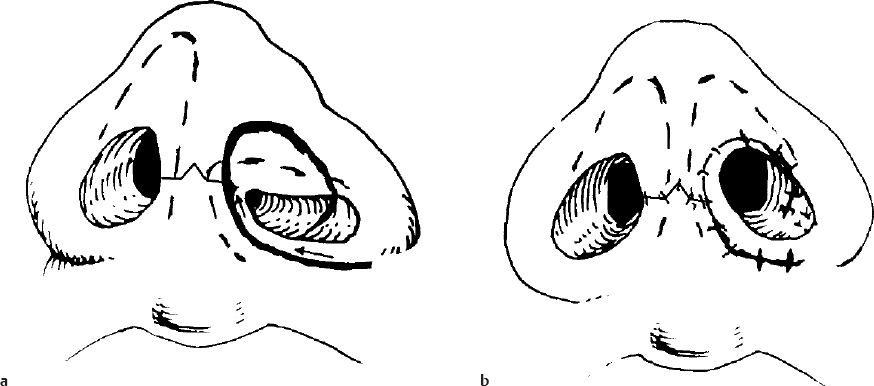
One of the hallmarks of cleft nasal deformity is significant deviation of the nasal bones and septum. Many of the same techniques used in cosmetic or functional rhinoplasty are needed in definitive cleft rhinoplasty: osteotomies, dorsal reduction, submucous resection or the Metzenbaum “swinging door” septoplasty, spreader grafts, and onlay grafts. The crooked nasal deformity can be addressed with traditional techniques, but a few alterations have described. In 1930, Blair described repositioning of the entire dorsal complex while preserving the dorsal contour. This involves lateral osteotomies and a percutaneous osteotomy at the nasal root, with control of the lower nasal third by securing a mobilized caudal septum to the periosteum of the anterior nasal spine ( Fig. 10.2 ).
The caudal septum is typically deviated toward the noncleft side, but variations of septal deformities have been described.22 If a reduction in dorsal projection is desired, layered lateral osteotomies can be done to allow the bones to telescope and thus de-project the entire nasal dorsal complex. Alternatively, many surgeons are adept at direct dorsal hump reductions with completion lateral osteotomies as a means to repositioning the bony pyramid. Specific to the cleft nasal deformity, Cutting23 and others14,16 highlight the importance to disarticulate the ULCs from the dorsal septum and use asymmetrically sized spreader grafts to stent the nasal airway and help straighten any curvature of the dorsal septum.
Skin Envelope
Correction of the soft tissue abnormalities found in the mature cleft nasal deformity is one of the most difficult tasks and a prominent rationale to pursue primary cleft rhinoplasty.6,24 Some findings include the following: (1) the skin over the cleft-side nasal tip is flat, (2) an amorphous deposition of fibrofatty tissue in the interdomal space, (3) a web or hooding at the cleft-side soft tissue triangle, and (4) the cleft-side vestibular lining at the plica vestibularis is irregular and under more tension than the normal side.
Among the anatomic deformities found in the cleft nose, there is disagreement as to whether there is a true soft tissue deficiency on the cleft side at birth or whether it is a case of soft tissue malposition over abnormal framework.25 As the child grows, these asymmetries become more prominent. Atherton presented histologic evidence that nasal cartilage on the cleft side was similar to the noncleft side in all dimensions,26 although this study was in the fetus, and not after completion of nasal growth. In the mature patient with cleft nasal deformity, however, there is often a presumed soft tissue deficiency of the vestibular lining. In fact, many of the current surgical techniques address this problem through different strategies. So although the cartilage framework is not deficient at birth, it is believed that the combination of prior surgical scarring and worsening malposition of the underlying framework ultimately restrict soft tissue development by the time of complete nasal maturity. There is greater consensus that in bilateral cleft nasal deformity there is a true deficiency in vestibular lining and columellar skin.27,28
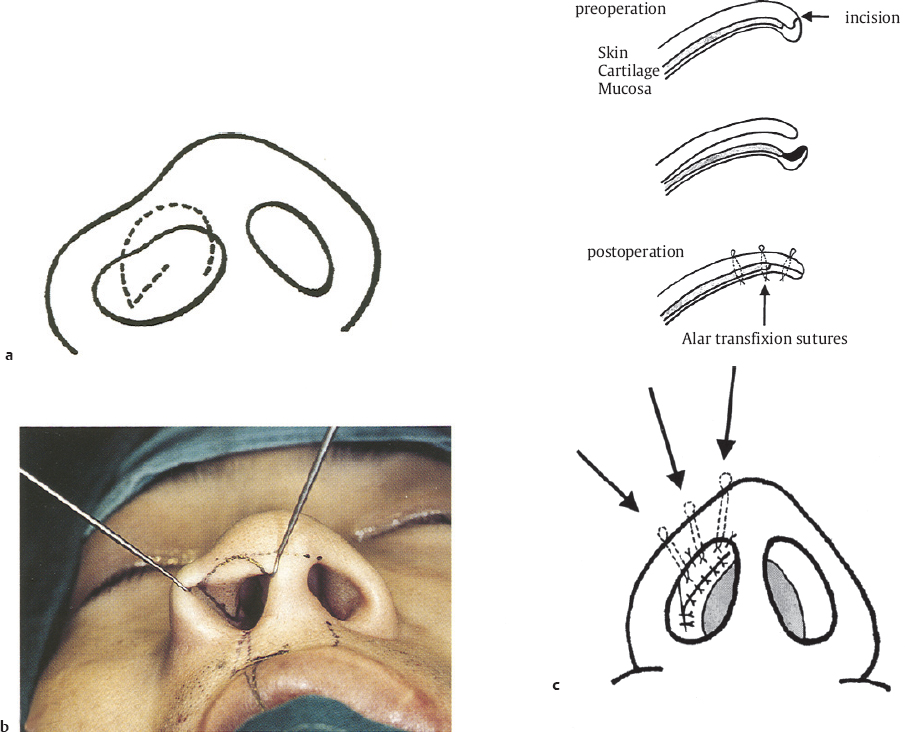
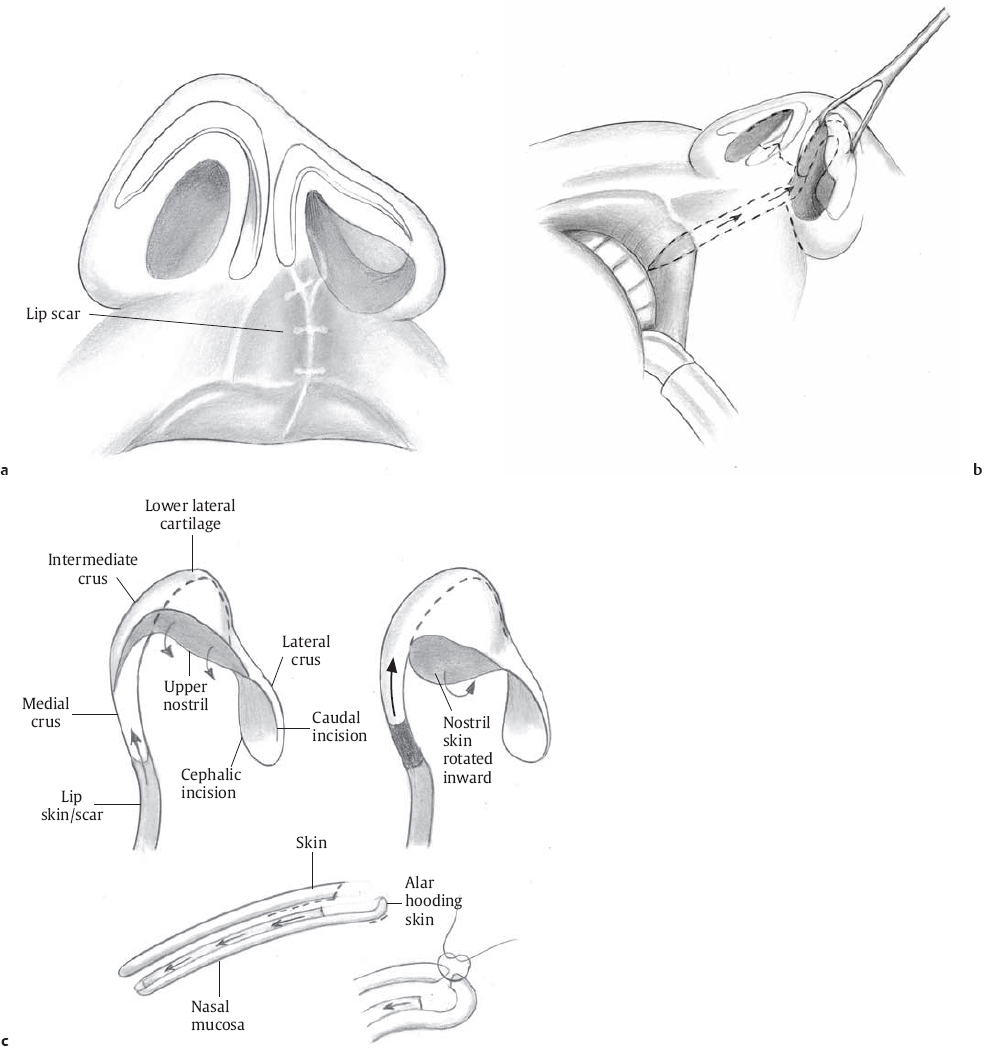
The deficiency in vestibular lining can be categorized as either in a transverse (horizontal) or longitudinal (vertical) vector. Tajima′s reverse-U incision introduces new vestibular lining predominantly in the longitudinal vector by moving external alar rim skin into the vestibule as part of LLC repositioning. The nasal alar hooding is improved by internally rotating the external skin of the soft tissue triangle into the nostril ( Fig. 10.3 ).29
The incision along the caudal margin of the cleft-side alar cartilage is extended out onto the hooded alar rim skin at the point of greatest deformity (hooding). The amount of lining introduced into the vestibule is dependent on the amount of hooded skin at the ala rim. Cutting, Bardach, and Pang note that horizontal lining deficiency is challenging to repair, and explains how its origin can be traced back to the alar base repositioning done during primary lip repair. A small nostril aperture is created when the cleft-side dome cartilage and lateral crura are left underprojected and the alar base is medialized.6 By the time of nasal maturity, the vestibular lining on the cleft side is constricted; ultimately, there is lining deficiency at the dome, the alar rim, along the nasal floor, and mucosal tension over the plica vestibularis.
The modified Vissarionoff sliding cheilorhinoplasty (SCR) is another technique that introduces internal lining in a transverse orientation.30 The upper lip scar from the original lip repair is left attached to the skin over the medial crus (a chondrocutaneous flap). This flap slides into the nose and is advanced around the contour of the LLC ( Fig. 10.4 ). The lining is delivered to the area where most secondary rhinoplasty patients have deficiency: along the columella and at the dome in a transverse vector. The amount of skin introduced is limited by the width of the lip scar and the anterior projection of the cleft-side medial crura during cartilage repositioning. This technique can be combined with the reverse-U incision to gain further internal lining.
Other methods to increase internal lining include full thickness grafts31 or auricular composite graft32 to the lateral wall defect after medial repositioning of the cleft-side lateral crura. These techniques can introduce a significant area of vestibular lining but can have drawbacks—the healed skin graft site can show a marked depression and does not provide support against contracture, while the viability of a free composite graft is more tenuous and can heal with a thickened scar. Alar hooding is a soft tissue deformity along the medial aspect of the alar rim, as mentioned previously. The standard description for the cause of the alar hood is from displacement of the alar base causing a posterolateral pull on the alar margin and secondary webbing at the soft tissue triangle.
The etiology of alar hooding is further described by Agarwal and Chandra.33 The LLC attachments are abnormal in the unilateral cleft nose and preclude caudal descent, including (1) the interdomal ligament, (2) anteroinferiorly to the caudal septum, and (3) superiorly at the scroll to the ipsilateral ULC. The dilator naris anterior and compressor nares muscles were found to be hypertrophic and the cleft-side lateral crura wider compared to the contralateral normal side. Agarwal and Chandra reasoned that the muscles exercise differential pull on the cartilage resulting in the overgrowth and prolapse of the alar cartilage into the soft tissue triangle area, an area where the cartilage meets with minimal resistance. To correct this problem, Agarwal and Chandra suggest sliding some of the skin internally, then partial excision of the remaining skin and the portion of cleft-side lateral crural “overgrowth” present in this area.
Other strategies include Tajima′s reverse-U incision as described, which relies predominately on repositioning both cartilage and skin. In China, Wang and Fan introduced a technique to address soft tissue deficiency at the nostril sill while simultaneously removing alar hooding.34 A narrow laterally based transposition flap of skin and fibrofatty alar tissue is harvested from the alar hood and rim, pedicled at the alar base, and inset into the nasal sill. If the alar base is too lateral, the flap can be inset in the crescent-shaped defect along the neo-alar groove after medialization of the base. While this flap may be useful in some circumstances, it comes at the cost of extensive scars placed in highly visible areas that have a tendency for hypertrophic scarring.
Repositioning of Nasal Tip Cartilages
Much of the debate in the cleft rhinoplasty literature has centered on differing philosophies of what soft tissue and nasal cartilage needs to be repositioned and how best to do it. As mentioned, there are a multitude of anatomic deformities of the cleft-side nasal cartilages, including retrodisplacement and underprojection of the dome on the cleft side, lateral slumping of the cleft-side medial crus, and a lateral intranasal wall fold called the plica vestibularis. Despite the opinions on how to address the problems, it seems clear that repositioning and reshaping of the cleft-side cartilages is necessary to restore form and function. Although traditional suture modifications of the native nasal cartilages have been described in Chapters 4, 5, and 6,35 an open rhinoplasty approach to mobilize cartilage and reposition is more common. In general, there are two basic approaches: those techniques that move the cleft-side LLC from medial to lateral, and those that move the LLC from lateral to medial.
Medial-to-Lateral Cartilage Repositioning
These authors support the medial-to-lateral LLC repositioning approach using a technique termed the sliding chondrocutaneous flap or SCR.2,15,30 This approach represents an evolution of techniques over many years. In 1932, Gilles described a composite chondrocutaneous hemicolumella flap using a mid-columellar incision and advancement superiorly.30 In 1964, Converse modified this technique by using a midcolumellar incision joined to a marginal incision. Once the LLC composite graft was advanced and the cleft-side medial crura secured to the contralateral dome, the skin and vestibular defect was repaired with an auricular composite graft.36 Dibbell introduced a variation on this theme by creating a bipedicled flap beginning on the nasal floor skin, which is elevated in continuity with cleft-side medial crura.37 The composite flap is rotated clockwise around the cleft-side vestibule, with the medial crura further projected, the entire cleft-side cartilage repositioned, and the alar base carried medially by the bipedicled nasal floor flap. Cutting describes how to combine the Dibbell rotation technique with Tajima′s reverse-U incision using an external rhinoplasty approach ( Fig. 10.5 ).38
In an effort to correct the vestibular lining deficiency, Vissarionov showed in 1989 how the skin from the upper lip cleft repair scar could slide up to replace the vestibular lining defect instead of rotating nasal floor tissue up into the dome or using a composite graft from the ear.39 Soon afterward, Vissarionov′s technique was combined with the external rhinoplasty approach by melding the incisions needed for the SCR flap together with a transcolumellar incision and contralateral marginal incision.30
The modern version of this SCR offers many advantages. The external rhinoplasty approach affords greater access for a variety of open techniques and structural grafting depending on each patient′s functional and aesthetic needs. A laterally based chondrocutaneous flap introduces new internal lining in a transverse vector to the vestibule while allowing for revision of the lip scar at the same time. The incisions can easily be adapted to combine Tajima′s reverse-U incisions for treatment of alar hooding and introduction of more internal lining in a longitudinal vector ( Fig. 10.4 ).
The SCR can be used whether the alar base is too medialized or lateralized. If the base is too narrow, V-Y sulcus advancement is done with the distal end of the chondrocutaneous flap placed within the sill soft tissue defect. If the base is too lateral, then the alar base is medialized during the lip revision by anchoring a key stitch from the alar base to the periosteum of the anterior nasal spine.
Key indications for SCR for secondary correction of the unilateral cleft nose include the following:
Moderate to severe cleft nasal nose with multiple deformities present
Mild to severe vestibular lining deficiency
Unfavorable lip scar; need for lip revision
Need for structural grafting (i.e., spreader grafts, columellar strut, batten graft)
An outline of the operative technique for SCR has been described previously,8 and is presented here in detail ( Fig. 10.6 ). The cleft lip scar on the upper cutaneous lip is used as part of a composite advancement flap. This technique works best when the scar is linear or curvilinear, which is the typical result after a Millard-type, rotation-advancement style lip repair. It is still possible to use this technique in those who have had geometric style lip repairs, although the scar is usually greater in horizontal dimension, making it more difficult to mobilize the entire scar as part of a chondrocutaneous advancement flap without further narrowing the white lip. The purpose of advancing the lip scar into the nose is to correct any deficiency of vestibular lining at the dome.
The design of the transcolumellar, inverted-V incision for the external rhinoplasty approach is placed at the narrowest point of the columella. The vermilion cutaneous border and the lip scar are outlined with methylene blue tattoo markings. If there is alar webbing on the cleft side, markings are designed on the external nasal skin at the alar rim to create symmetry for the nostrils and alar rims using the noncleft-side alar rim as a guide. These skin markings are curved back into the vestibule medially and laterally to be continuous with a marginal incision along the caudal border of the cleft-side lateral crura. The width of the lip scar marking is specific to each patient, but typically is a long narrow ellipse at least 5 mm in width that extends down to the vermilion border. Over the red lip, the amount of vermilion excised is tailored to the individual based on what is needed for the most favorable aesthetic outcome. The lip scar markings extend into the nose along the medial vestibule. The medial edge of the lip scar marking is joined to the vertical component of the marginal incision used in the standard external rhinoplasty approach. If there is alar hooding, the marginal incision leaves the caudal border of the cleft-side lateral crura to incorporate external nasal skin that was causing hooding, then merges back into the lateral vestibule to complete the marginal incision ( Fig. 10.6b,c ).
The versatility of the SCR allows for two distinct sources of skin to introduce vestibular lining to the cleft side while simultaneously correcting unfavorable lip scars and any alar web deformity. The lateral edge of the lip scar marking continues into the medial vestibule as a vertically oriented incision along the anterior septum that continues superiorly and laterally as an intercartilaginous incision. Care must be taken to keep the lateral attachment of the cleft-side lateral crura intact in order to maintain the blood supply to this chondrocutaneous flap.
The initial incisions around the lip scar begin at the lip and extend to the nose in a subdermal plane. The intranasal vestibular skin is incised along the previous markings. As the lip scar skin flap reaches the base of the columella, the depth of dissection is deepened to incorporate the cleft-side medial crura as a chondrocutaneous flap. This plane of dissection is continued over the cleft-side dome and lateral crura. The chondrocutaneous flap blood supply comes from the intranasal attachment near the cleft-side piriform aperture. The inverted-V columellar incision is made and standard external rhinoplasty approach is completed to expose the nasal cartilages and dorsum. Correction of the nasal septum is done via the external approach by division of the interdomal ligament and separation of the ULCs from the anterior septum. Septal cartilage is harvested for grafting and repositioning the caudal septum over the nasal spine. Structural grafting (e.g., spreader grafts, lateral crural strut grafts, alar rim grafts) and osteotomies can be completed next.
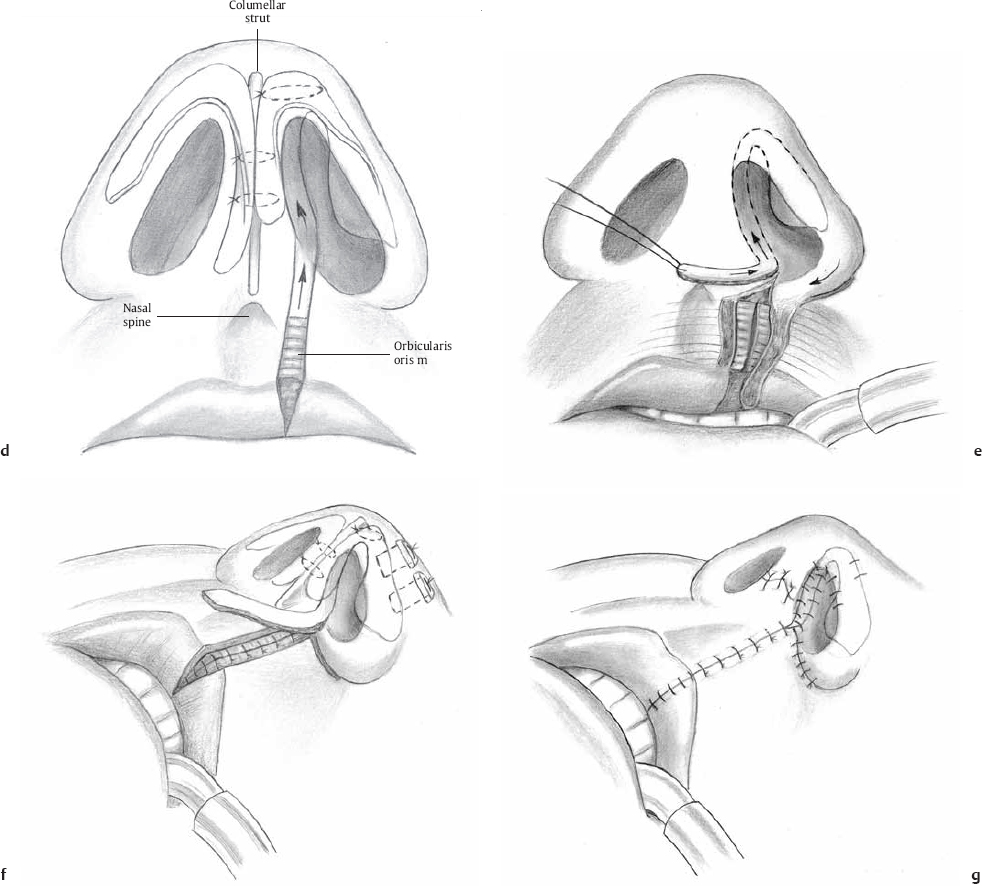
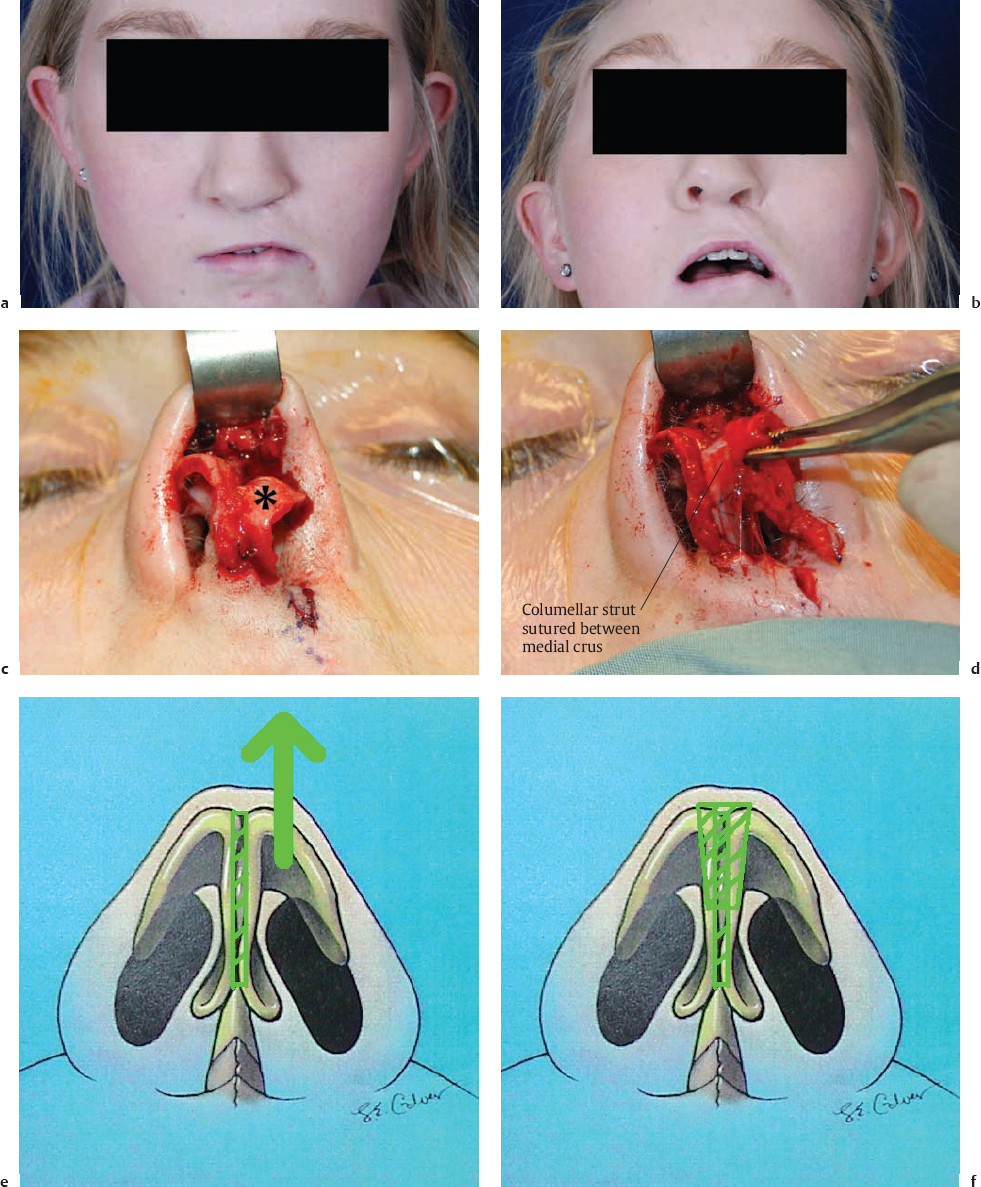
A columellar strut is often used to suspend the medial crural cartilages using harvested septal cartilage, auricular cartilage, or costal chondral cartilage. A precise soft tissue pocket is developed between the medial crura, which are then anchored to the columellar strut ( Fig. 10.7a–j ). The critical part of the cleft-side nasal cartilage repositioning is how much advancement is needed for the cleft-side medial crura so that the vestibular dome heights are symmetric. To evaluate the nasal tip symmetry, a 25-gauge needle is placed between the medial crura and columellar strut complex. At this point in the case, the height of the vestibular mucosa at the new domes is used as a reference point for dome symmetry rather than the nasal cartilages themselves. A plain gut suture on a straight needle is passed through the entire columellar complex in horizontal mattress fashion. As the medial crura and lip skin slide up toward the dome, this advancement acts like a “medial crural steal” procedure. To create dome symmetry at the cartilage level, the angle of domal divergence on the cleft side usually has to be made more acute with a dome binding stitch or other suture modification. Alternatively, cartilage-incising techniques such as vertical dome division can also be utilized to ensure dome symmetry. The superior half of the soft tissue triangle (nostril shape) has been sculpted at this point.
Next, the lip reconstruction and alar base repositioning is completed ( Fig. 10.6d ). The orbicularis muscle is reapproximated with deep buried stitches. If upper lip malalignment exists, rotation of the lateral-side muscle can be done similar to primary cleft lip repair. If excessive lateral position of the alar base is present—which is often a hallmark of the cleft nasal deformity—then the soft tissue attachment of the alar base to the premaxillary is released sharply and the lateral side muscle is advanced toward the nasal spine. In both settings, a vertically oriented “keystone” stitch is placed through the orbicularis muscles on the lateral side and the periosteum of the nasal spine on the medial side (see Fig. 4.12, Fig. 4.16b, and Table 5.1). Medialization of the alar base with this suture allows for sculpting of the inferior half of the nostril shape. The alar base width can be measured from the middle of the columella on the normal side as a guide for how tightly to narrow the alar base on the cleft side. The medialized soft tissue bulk of the alar base can also serve to provide some augmentation to the nasal sill, which is often deficient in the setting of alveolar ridge and palatal clefts. With the tension on the closure borne by the muscle, the skin edges are meticulously reapproximated with maximal skin eversion, which can improve ultimate scar appearance.

After the nasal base volume and width are corrected, refinements to the nasal tip are performed. These maneuvers are specific to the needs of each patient, and include cephalic trims of the LLCs, a shield-type tip graft, and cap grafts. In the cleft nose, these authors believe that the combination of congenital soft tissue envelope thickening and scarring from prior surgical intervention make tip refinement more consistent with grafting rather than suture modification alone. Furthermore, the external rhinoplasty approach allows for many of the remaining cleft deformities to be treated with some additional modifications. For example, the plica vestibularis deformity is caused by deficient support from the lateral scroll, inherent paradoxical curvature of the cleft-side lateral crura, and tension on the lateral crura from horizontal lining deficiency. An alar batten graft can brace and straighten the cartilage along with suture suspension of the LLC to the ULC ( Fig. 10.8 , graft not shown). When using a laterally based intranasal chondrocutaneous flap, an underlay lateral crural strut graft is contraindicated because the vestibular lining needs to stay attached to the lateral crura to maintain blood supply to this laterally based flap.
To correct the deficient scroll support, the traditional Skoog-type suspension sutures go from the cephalic edge of the cleft-side lateral crural to the ULC and nasal dorsum.14 The medial and cephalic suspension sutures proposed by Tajima in the “reverse-U” approach can also be done at this time, depending on patient need and surgeon preference ( Fig. 10.8 ). During closure, the reverse-U component of the chondrocutaneous flap at the alar rim can be contoured as needed to introduce whatever component of vestibular deficiency was present as well as obtain symmetry of the alar rim position.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


