Fig. 1
(a–c) Non-weight-bearing clinical photographs. Note the rotational deformity that has caused the infected wound at the base of the residual fourth metatarsal

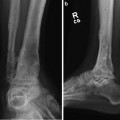
Fig. 2
(a–e) Pre-operative reformatted CT images reveal the rotational deformity that has developed between the hindfoot and forefoot at the tarsal-metatarsal junction

Fig. 3
Using the 3D model from the CT scan, a three-dimensional wedge of bone is removed at the apex of the deformity. In this varus-supination deformity, the wedge will be larger dorsally and laterally, being centered at the CORA

Fig. 4
A pre-built three-level static frame is used for maintaining the surgically obtained correction. Note that the proximal ring can be changed out for a ring one diameter size larger to accommodate for the calf muscles

Fig. 5
The pre-built three-level circular frame is placed on the limb (see text)
3 Preoperative Problem List
1.
Recurrent weight-bearing wound with underlying osteomyelitis.
2.
Residual forefoot varus secondary to the motor balance that developed following the initial fifth ray resection. The ray resection allowed a motor imbalance from an unopposed posterior tibialis muscle. The resulting deformity could not be accommodated by orthotic methods.
3.
Motor imbalance between the foot and ankle dorsiflexors and plantar flexors secondary to the motor peripheral neuropathy. An important component of the pathophysiology associated with Charcot foot arthropathy is the muscle imbalance created by the motor peripheral neuropathy that affects small nerves (and, hence, small muscles) earlier in the disease process than larger nerves. This motor imbalance is expressed clinically by the larger ankle plantarflexors overpowering the smaller and weaker dorsiflexors.
4 Treatment Strategy
1.
This motor imbalance of the gastrocnemius-soleus overpowering the dorsiflexors is addressed by either percutaneous tendon Achilles lengthening or gastrocnemius musculotendinous lengthening.
2.
This specific patient also has a motor imbalance between the invertors (posterior tibialis) and the disengaged evertor (peroneus brevis). This motor imbalance is addressed by a fractional muscle lengthening of the posterior tibialis at the musculotendinous junction.
3.
4.
The dynamic deformity was addressed by muscle-balancing surgery. The static structural deformity was addressed by the wedge-resection osteotomy. Thus, the deformity was acutely corrected at the time of surgery. Following removal of the wedge of bone, the rotational component of the bony deformity can be corrected and provisionally maintained by percutaneous smooth wires.
5.
The surgically obtained correction was maintained by applying a pre-constructed three-level circular external fixator (Fig. 4). Note that the most proximal ring can be “up-sized” by one ring diameter to accommodate the larger calf muscle.
6.
In order to augment the stability fixation of the re-aligned foot, static fixation is accomplished in stages. The hindfoot is secured to the foot ring via two olive
 8: Femoral Bone Defect
8: Femoral Bone Defect
 11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
 22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
 39: Ilizarov Ankle Fusion
39: Ilizarov Ankle Fusion
 84: Lapidus Fusion with External Fixation
84: Lapidus Fusion with External Fixation
 65: Closed Correction of Club Foot with Ilizarov
65: Closed Correction of Club Foot with Ilizarov




Related posts:
8: Femoral Bone Defect
11: Bone Transport Over a Nail for Infected Tibial Nonunion and Bone Defect
22: Bone Transport to a Knee Fusion and Secondary Intramedullary Nailing s/p Gunshot Wound
39: Ilizarov Ankle Fusion
84: Lapidus Fusion with External Fixation
65: Closed Correction of Club Foot with Ilizarov
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
