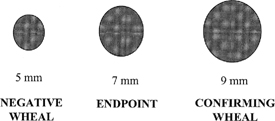
4 Intradermal testing using varying dilutions of antigens has been the cornerstone of skin testing in otolaryngic allergy for over a half century. Reliance on the methodology of intradermal dilutional testing (IDT) demands an understanding of the normal and abnormal responses to intradermal skin testing in allergic and nonallergic individuals. In this era of evidencebased medicine, it is unfortunate that much of our information is still based on the reported anecdotal experience of Herbert Rinkel. Fortunately, he proved to be a very astute observer, and most of his recommendations have stood the test of time thus far. Cooke,1 whowas a pioneer in the area of intradermal testing, thought that a proper intradermal injection of 0.01 cc should produce a wheal of 2 to 3 mm in diameter. This belief was echoed by Rinkel’s mentor, Dr. French Hansel.2 However, Rinkel observed that the injection of 0.01 cc, when “truly intracutaneous,” formed a wheal 4 mm in diameter, a papule that was pale and sharply demarcated with abrupt edges. Furthermore, when there was no antigenic response, this 4-mm wheal usually enlarged to a diameter of 5 mm at the end of 10 minutes, although it would sometimes reach 6 mm in size.3 An increase of the wheal to 7 mm or greater in diameter (i.e., 2 mm larger than the typical negative 5-mm wheal) was thought by Rinkel to indicate an allergic reaction, and was interpreted as a positive response. Furthermore, Rinkel found that if he applied an intradermal test with antigen that was yet five times stronger, the resulting wheal was 2 mm or more larger than the preceding positive wheal. Although allergists had for decades used 10-fold dilutions in treatment, Rinkel thought that fivefold dilutions offered distinct advantages. First, he noted the increment in the whealing response to be constant through three or four consecutive dilutions in almost three quarters of patients tested. In addition, he found that treating using fivefold dilutions carried less risk of overdosing in going to the next stronger treatment vial.3 Rinkel called the antigen strength producing the first positive response the “endpoint of titration,” signaling the concentration at which immunotherapy could safely be initiated. The next stronger concentration, producing yet a larger positive wheal, he termed the “confirming wheal.” The importance of testing to obtain a confirming wheal lies in conclusively demonstrating that the endpoint concentration has initiated progressive positive whealing, establishing that one is dealing with a true endpoint. Antigens are prepared in fivefold dilutions, beginning with a concentrate. For years, almost all antigens were designated in weight per volume (w/v) strengths, and most otolaryngic allergists employed a 1 : 20 w/v strength as concentrate. By convention, dilution No.1was a 1 : 100 solution, No. 2 was 1 : 500, and so forth to No. 6, or 1 : 312,500. Now many antigens are available as standardized solutions, but the convention of naming test concentrations by how many times they have been diluted is still followed. Although Rinkel often began testing with extremely dilute antigen concentrations, based on studies using direct immunoglobulin E (IgE) assay by radioallergosorbent test (RAST) methods, it has been determined that it is rarely, if ever, necessary to begin testing and treatment with concentrations weaker than a 1 : 312,500 weight/volume solution (i.e., a No. 6 dilution). In allergy testing, enlargement of a 4-mm-diameter intradermal wheal beyond normal physical spreading to 5 mm is due to a reaction between the injected antigen and mast cells in the skin with specific IgE for that antigen fixed to them. The antigen reacts by bridging two adjacent IgE molecules, resulting in mast cell dissolution and the release of preformed and newly formed mediators of inflammation. After ~5 minutes, swelling of the skin begins due to increased vascular permeability, producing the “wheal” response. The size of the wheal is proportionate to the amount of mast cell activation, and it is considered to be an indicator of the amount of IgE-mediated release of mediators from mast cells. Other mediators, including substance P and platelet-activating factor, cause local erythema, the “flare” seen around some skin tests. The wheal reaches its maximum at 10 to 15 minutes, although the wheal and flare may persist to some degree for some time thereafter.4
Whealing Responses to Intradermal Testing: The Basis for Intradermal Dilutional Testing (IDT)
Richard L. Mabry
♦ Historical Background
♦ Antigen Dilutions
♦ Normal Whealing Responses
Whealing Responses to Intradermal Testing: The Basis for Intradermal Dilutional Testing (IDT)
Only gold members can continue reading. Log In or Register to continue





Full access? Get Clinical Tree


