7 Trichloroacetic Acid (TCA) Peels
Introduction
Chemical peels have been documented in American medical literature since Eller and Wolff described their use for treatment of blemishes and pitted scars of the face in 1941. Since that time, physicians have expanded the indications for chemical peels and advanced the understanding of the physiologic effect of these agents. Chemical peels are now commonly used to remove damaged skin and to promote regeneration and improvement in quality and overall texture of the skin. Chemical peels are classified according to their depth of penetration. Superficial peels are those reaching, at greatest depth, the superficial papillary dermis. Medium-depth peels are those reaching the papillary to reticular dermis, and deep peels extending to the mid-reticular dermis. Trichloroacetic acid (TCA) may be used for tissue penetration of superficial and medium-depths, depending on the concentration (Table 7.1). For superficial peels, TCA should be between 10% and 25% concentration. For medium-depth peels, most experienced physicians will use a concentration of 35% combined with another agent, and no greater than 40% since concentrations of 50% are known to impart a much greater risk of scarring, pigment dyschromia and undesired textural change. See Box 7.1.
Table 7.1 Chemical peel agents
| Peel type | Agent |
|---|---|
| Superficial | TCA 10–25% Jessner’s solution Glycolic acid |
| Medium | TCA 35–50% Solid CO2 + TCA 35% Glycolic acid 70% + TCA 35% Jessner’s solution + TCA 35% |
| Deep | Phenol peel |
Selection of Peel Type
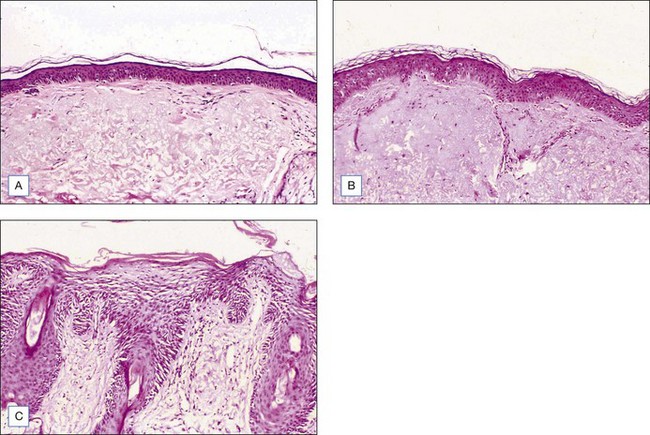
Choosing the correct concentration for the desired indication in any one patient requires consideration of the following factors: what is desired by the patient, photoaging classification by the physician, Fitzpatrick sun-reactive skin type classification, sebaceous quality of the skin, presence of inflammation (seborrhea, retinoid dermatitis, etc.), and skin translucency. (The more translucent the skin and more inflammation present, the more likely the patient will convert from a superficial to a medium-depth peel.) Indications for superficial peels include treatment of melasma, comedonal acne, and improvement of overall skin reflectiveness, texture, and tone. The use of superficial peels for actinic damage is controversial and some studies suggest that the improvement of actinic damage using superficial peels is no greater than that achieved by using topical glycolic products or topical retinoids alone. Indications for a medium-depth peel include reversal of actinic damage, including removal of actinic keratoses and other epidermal lesions, reduction of rhytides, removal of dyschromia, and improvement of atrophic scarring (Figs 7.1 and 7.2).

• Superficial peels
For superficial peels, patients who belong to Glogau classification for photoaging types I and II are most appropriate (Box 7.2). Severe photodamage with resultant hyperkeratosis and parakeratosis creates a barrier to peel penetration and will minimize the effect of any peeling agent. This can make using only a superficial peeling agent almost totally ineffective. It is therefore recommended that a retinoid be used to pretreat the area and increase the penetration of the peel. With regards to sun-reactive skin types, Fitzpatrick types IV, V, and VI are most prone to developing postinflammatory hyperpigmentation (Table 7.2). Pretreatment with tretinoin and hydroquinone may minimize this effect and can be particularly helpful in type IV, where the hyperpigmentation may be the most noticeable compared to their normal skin tone. Topical ascorbic acid has also been used as a priming agent and has been found to be beneficial in decreasing pigmentation. Soliman et al (2007) reported a significant improvement in melasma patients who were pretreated with topical 5% ascorbic acid prior to a superficial peel with 20% TCA. With adequate patient education, patients with darker complexions can safely undergo superficial peels without risk of permanent color change as hyperpigmentation fades over time and with treatment. Oily, thickened, sebaceous skin may lead to uneven and less effective superficial peeling. Peel response may be improved with the use of pretreatment tretinoin on a daily basis combined with alpha-hydroxy acids (10–20%) used as a daily cream, lotion or gel. In addition, a more vigorous skin preparation may be used to enhance peel absorption. In contrast, there are patients, usually women, who have paper-thin skin with a translucent quality. These patients are at an increased risk for conversion to a medium-depth peel with superficial peeling agents and should have their skin preparation and skin pretreatment performed cautiously. Other patients who deserve caution are those with seborrhea and other types of dermatitis (retinoid, etc.) Inflammation in the skin is known to enhance uptake of the peel solution and result in a deeper than expected peel.
Box 7.2
Glogau’s classification of photoaging
Based on Glogau (1994)
Table 7.2 Fitzpatrick’s classification of sun-reactive skin types
| Skin type | Color | Reaction to first summer exposure |
|---|---|---|
| I | White | Always burn, never tan |
| II | White | Usually burn, tan with difficulty |
| III | White | Sometimes mild burn, tan average |
| IV | Moderate brown | Rarely burn, tan with ease |
| V | Dark brown* | Very rarely burn, tan very easily |
| VI | Black | No burn, tan very easily |
* Asian Indian, Oriental, Hispanic, or light African descent, for example
• Contraindications
In addition to choosing the right patient with reasonable expectations for the procedure, complications may be avoided by excluding patients under certain circumstances. Relative contraindications for chemical peels include the use of isotretinoin (should be off it for at least 6–12 months), a history of radiation to the region (ablating adnexal structures), active herpes simplex or bacterial infection, history of hypertrophic scar formation, and a rhytidectomy or brow lift in the previous 3 months. With regards to brow lift and rhytidectomy, while waiting 3 months for resurfacing has traditionally been recommended, a publication by Alster et al (2004) described 34 patients who underwent combination carbon dioxide (CO2) or erbium:yttrium-aluminum-garnet (Er:YAG) laser skin resurfacing and surgical lifting procedures (S-lift rhytidectomy, blepharoplasty, and brow lift). The effects were found to be no different than those in patients undergoing the laser-only procedure. An article by Herbig et al (2009) suggests that the same may be true for chemical peel resurfacing. They reported performing 27 face and/or neck lifts with SMAS plication or SMAS-ectomy along with full face chemical peels and noted no hypertrophic scarring. Certain facial surgical procedures utilizing a skin or muscle flap may still compromise vascular supply to the tissue and result in delayed healing following medium-depth peels. Patients with a history of herpes simplex virus infection should be pretreated with an oral antiviral agent, which is continued until reepithelialization occurs.








