(1)
Department of Dermatology, Drexel University, Philadelphia, Pennsylvania, USA
Abstract
Eczema is one of the most steroid-responsive dermatoses. A midpotent corticosteroid preparation will generally suppress the inflammation and clear the rash. If the condition has not improved substantially within 2–4 weeks, a more potent corticoid may be selected. Topical antibiotics such as mupirocin may be used for significant crusting and exudation. Antibacterial compounds or maneuvers such as bleach gels, bleach baths, iodinated ointments, and quinoline-containing ointments may also be used to good effect. Oral antibiotics may be prescribed, but the resident staphylococci are multidrug resistant. The topical antibacterial approaches are conceptually better in light of the concept that staphylococci and their biofilms play the major role in this disease. These organisms are part of the normal flora, so even if they are killed, they will return at some point. Heresy enters the discussion of treatment regarding skin care during and especially after the rash. Even though we believe the rash is initiated by staphylococci and their biofilms occluding the sweat ducts, it is easier to help prevent the disease by treating the genetic component of the condition. This is done by treating the skin exceedingly gently and severely limiting soap, hot water bathing, frequent bathing, and scrubbing. Aggressive moisturizing is also needed. Azathioprine, methotrexate, or another immunosuppressive agent may be needed in severe cases.
Keywords
AntibacterialsAntibioticsCorticosteroidsMoisturizationSkin care Staphylococcus The many types of eczema that are encountered include flexural, facial-extensor, nummular, pityriasis alba, lichen planus–like, and mycotic (Figs. 7.1, 7.2, 7.3, 7.4, 7.5 and 7.6).






Fig. 7.1
Flexural eczema. In the antecubital fossae are large, dull, red and brown lichenified plaques that contain excoriated papules and eroded vesicles
Fig. 7.2
Facial-extensor eczema. On the lower legs and feet are hyperpigmented, excoriated, eroded, and scaling plaques. Onychomycosis is also evident
Fig. 7.3
Nummular eczema. On the lateral abdomen is a solitary, hyperpigmented, lichenified plaque
Fig. 7.4
Pityriasis alba. Hypopigmented, nonscaling patches are present on this child’s face. An “allergic shiner” (red-brown focus of hyperpigmentation) is present beneath the eye; a Dennie-Morgan fold is also evident
Fig. 7.5
Lichen planus–like eczema. On this man’s thigh are many purple-brown, discrete and confluent scaling papules and plaques
Fig. 7.6
Mycotic eczema. On the lateral foot erythema is present in a moccasin distribution. Many pink papules and papulovesicles extend to the ankle. These were culture positive for Trichophyton rubrum
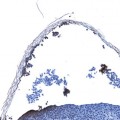
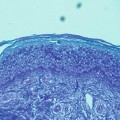
Physicians have long done an excellent job in treating eczema in all its presentations, for it is one of the most steroid-responsive dermatoses. What that implies is that any midpotent corticosteroid preparation (cream, ointment, lotion, spray, or foam) will generally suppress the inflammation that is so readily apparent in this disease, and clear the rash [1, 2] (Fig. 7.7). The “apparent” part is redness (erythema), edema, vesiculation, and excoriations (from scratching; this is the “itch that rashes”) [3]. Chronic forms of the disease show lichenification, or thickening of the skin with accentuated skin markings, along with the ever-present excoriations [3] (Fig. 7.8).


Fig. 7.7
Clearing of facial eczema with treatment and skin care. This child’s facial plaque (left cheek), which previously was papulovesicular and bright red, is now a red-brown patch with surrounding hypopigmentation. The treatment was triamcinolone ointment 0.1 % twice daily for 2 weeks. The mother followed bathing instructions literally
Fig. 7.8
Lichen planus–like eczema
Often the itch is so severe, scratching will occur even during the dermatologic examination. If the condition has not improved substantially within 2–4 weeks, a more potent corticoid may be selected [1, 2] (Table 7.1).
Table 7.1
Corticosteroids for eczema treatment
Class 1: superpotent (based on vasoconstriction) |
Clobetasol propionate 0.05 % cream, ointment, solution, foam |
Betamethasone dipropionate 0.05 % augmented (with propylene glycol) |
Halobetasol propionate 0.01 % cream, ointment |
Fluocinonide 0.1 % cream |
Class 2: potent |
Betamethasone dipropionate 0.05 % nonaugmented cream, ointment |
Mometasone 0.01 % ointment |
Fluocinonide ointment 0.05 % cream, ointment, gel, solution |
Halcinonide 0.1 % cream, ointment |
Desoximetasone 0.25 % cream, ointment |
Class 3: upper midstrength |
Desoximetasone 0.05 % cream |
Betamethasone valerate 0.1 % cream, ointment, foam |
Fluticasone 0.05 % ointment |
Class 4: midstrength |
Flurandrenolide 0.05 % ointment |
Mometasone cream 0.1 % |
Triamcinolone acetonide 0.1 % cream, ointment, solution |
Fluocinolone acetonide 0.025 % cream, ointment |
Hydrocortisone valerate 0.2 % cream |
Class 5: lower midstrength |
Flurandrenolide 0.05 % cream, lotion, tape |
Fluticasone 0.05 % cream, lotion |
Prednicarbate 0.1 % cream |
Desonide 0.05 % lotion |
Hydrocortisone butyrate 0.1 % cream, ointment, solution |
Hydrocortisone valerate 0.2 % cream |
Class 6: mild |
Alclometasone dipropionate 0.05 % cream, ointment |
Fluocinonide 0.01 % oil |
Fluocinolone acetonide 0.01 % cream, solution |
Class 7: less potent |
Hydrocortisone acetonide 1, 2.5 % cream, ointment, lotion, spray |
Hydrocortisone acetonide 0.5 % cream, lotion |
If used cautiously, even strong corticoids may be applied to sensitive areas of the skin. This is a relatively rare occurrence and fortunately the stronger corticoids are usually unnecessary. As the disease improves, less potent topicals, such as hydrocortisone acetate and calcineurin inhibitors, may be employed [2]. These latter agents may be used first if the disease is mild to moderate (Table 7.2).
Table 7.2
Corticoid regimens according to eczema severity
Ordinary presentation with good response |
Class 4 midpotency → class 7 with improvement → continue moisturizing |
Ordinary presentation with minimal response |
Class 4 midpotency → class 1 or 2 superpotent or potent → class 7 with improvement, continue moisturizing |
Mild presentation |
Class 7 less potent or calcineurin inhibitors → improvement → moisturize |
Impetiginized |
Class 4 midpotency plus topical antibacterials, moisturize |