25 Tower technique of filler injection
Summary and Key Features
• Previous injection techniques for facial rejuvenation aimed at simply ‘filling’ lines and furrows
• Volume loss has become an important hallmark of the aging face, thanks to greater knowledge and understanding of how we age
• New techniques focus on providing structural support and are performed vertically, rather than horizontally
• The tower technique features 90° injections with gradually tapering product deposition as the needle is withdrawn
• In the vertical supraperiosteal depot technique, small aliquots of filling agent are deposited on the periosteum for maximum support
• Softer hyaluronic acid formulations are recommended for more superficial injection, whereas more robust and cohesive products may be chosen for deeper implantation
Anatomical considerations
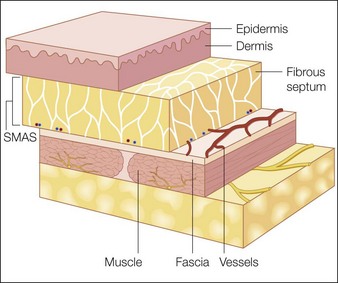
The facial skin and subcutaneous tissue (referred to as the soft tissue ‘flap’) comprise a dense, superficial formation of connective tissue that makes up the dermis and epidermis, a honeycomb web-like subdermal structure of connective tissue embedded in fat lobules, and muscle, which traverses the soft tissue flap (Fig. 25.1). Anatomical studies show that the immediate subdermal layer contains a large connective tissue network made up of small fat lobules with many septa, whereas the deeper subdermal layer features large fat lobules with only a few septa. Dynamic musculature presents in sometimes overlapping, multiple layers, and may even form entire complexes – as in the brow area where the frontalis, corrugator, and orbicularis muscles merge into one complex with the ability to move medially, proximally, and distally (F. Anderhuber, personal communication).
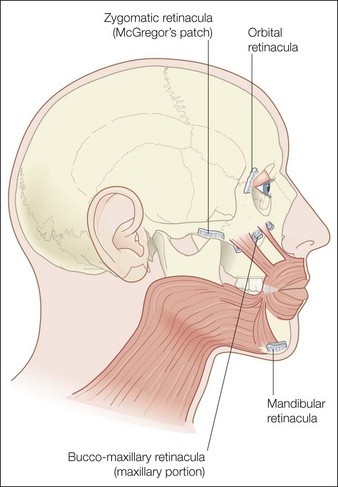
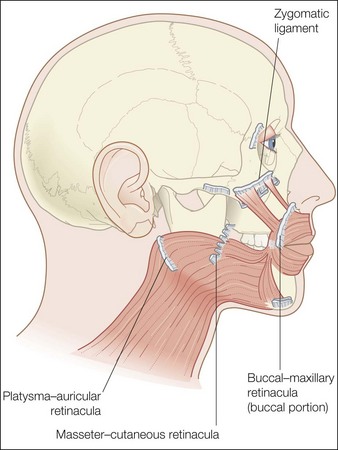
The analysis of the anatomical composition of the connective tissue is of greatest interest in volume augmentation. The soft tissue flap is attached to the underlying bony structure via connective tissue bands called retinacula or real retaining ligaments (Fig. 25.2), which show no or very limited elasticity. So-called false retaining ligaments – the most important of which include the nasolabial fold, the zygomatic ligament, and the maxillar–buccal ligament (Fig. 25.3) – add to the character of the flap surface. Although false retaining ligaments have no bony attachment, they act in a fence-like manner, compressing dynamic muscular activity and influencing the appearance, shape, and correction of the skin surface.
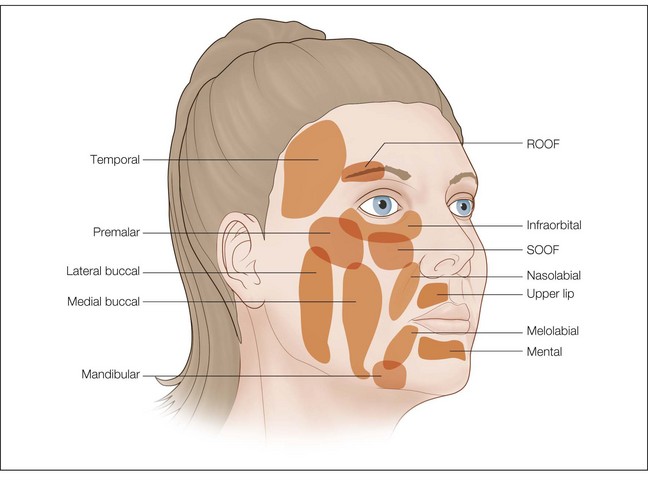
A brief description of the soft tissue anatomy of the human face is not complete without a discussion of the fat compartments, which are located around and below the eye, in the cheek, and in the perioral region (Fig. 25.4). The suborbicularis oculi fat (SOOF) and retro-orbicularis oculi fat (ROOF) pads are the dominant features of the periorbital region. As the most proximal entity in the mid-facial region with the least coverage of musculature structures, the SOOF pad plays a key role in the process of facial aging and has a direct impact on the clinical presence of the medial and lateral infraorbital hollow. Another important, shape relevant structure in the submalar area is induced by an indented groove from the medial orbital hollow to the lateral lower midface caused by the zygomatic ligament.
Biological characteristics of filler materials
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


