Chapter 13 Tissue and Fascial Expansion of the Abdominal Wall 
1 Introduction and Clinical Description
The abdomen lends itself to tissue expansion in patients of all ages and a multitude of clinical problems. Both congenital and acute defects of the abdominal wall can be addressed by the sequential expansion of adjacent tissues. These include the treatment of giant congenital nevi, tumors, burn scar contracture, posttraumatic defects, and loss of skin and fascial domain following previous surgery or injury. This chapter addresses the treatment of skin and sub-cutaneous tissue defects of the abdominal wall by utilizing prosthetic tissue expanders to both create new tissue and recruit tissue from healthy adjoining areas. It also discusses fascial expansion of the abdominal wall by the process of serial excision of a fixed prosthetic mesh. Because the anatomy of the abdominal wall is described elsewhere in this book, it is not repeated here.
1 Typical Skin Defect Requiring Tissue Expansion
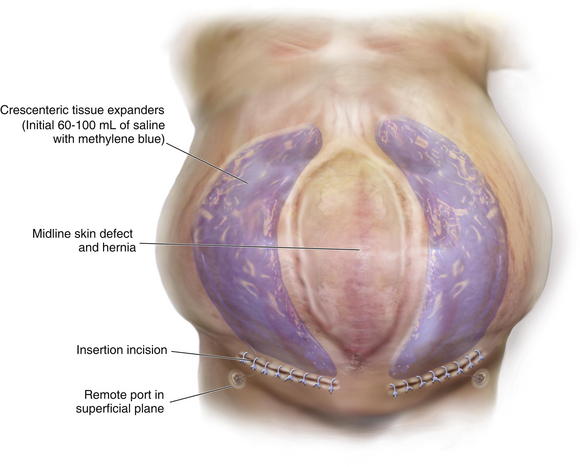
The typical defect that lends itself to repair via the insertion of tissue expanders is a well-defined defect that is well healed and stable (Fig. 13-1, A). Areas that have been irradiated or subject to diffuse trauma, such as burns and subsequent grafting and scar contracture, are less amenable to expansion. Open wounds or chronically draining wounds are also fraught with problems because of the high incidence of infection and subsequent extrusion of the expander. If a tumor is to be removed, there must be absolute certainty that the tumor is not contiguous with the tissue expanded pocket. In Fig. 13-1, A, a patient is shown with a large midline abdominal hernia and well-healed skin graft over bowel. The width of the graft is clearly too great to allow primary closure of the adjacent skin and subcutaneous tissues. He also has a large fascial defect, and if this is closed with prosthetic mesh, good skin closure over the mesh will be impossible. The shown defect will respond ideally to progressive expansion of bilateral crescenteric tissue expanders placed on either side of the central defect. The expanders are inserted on top of the abdominal wall fascia and completely underneath all of the skin and subcutaneous tissue lateral to the central graft and hernia. Over the course of several weeks to months, the expanders are filled with sterile saline via remote port. When they are deemed to be adequately expanded, they are removed in the operating room (OR), the central graft is excised, the hernia is repaired, and the skin flaps are advanced to the midline to adequately close the defect (see Figs. 13-2 and 13-5, p. 235).


2 Typical Fascial Defect Requiring Fascial Expansion
It is harder to define the typical fascial defect that will require or respond well to expansion via serial excision of prosthetic mesh. Frequently the type of procedure needed to close a fascial defect is not known until the hernia is dissected free during surgery, and the extent of the fascial loss or loss of domain is completely evaluated. In the patient shown in Fig. 13-1, B, on page 225, there is adequate skin coverage of the hernia, but there is a clearly massive hernia with obvious loss of abdominal domain. Approaches to the repair of this hernia include prosthetic or biologic mesh repair, separation of component parts repair, regional or free-flap reconstruction, or a combination of all three procedures. It is this author’s opinion that the best approach to abdominal wall reconstruction is to replace like with like and to return anatomic structures to their normal place. Thus, the ideal abdominal wall has innervated rectus abdominis muscles in the midline that contract during forced effort and help to maintain the integrity of the abdominal wall. To achieve this goal, the separation-of-parts procedure is ideal (see Chapter 8). Sometimes, however, the fascial defect is so large that the separation of parts is not sufficient. This is usually true if the defect exceeds 16 cm in width and the lateral abdominal wall is fixed and noncompliant. In this case the surgeon can attempt to bridge the defect with mesh (not an anatomic solution) or perform a staged procedure designed to gradually decrease the width of the fascial defect and reacquire abdominal domain. This multistage surgery involves three main components. The first is the initial operation where the hernia is dissected free, and the fascial defect is analyzed. At this time, a piece of nonadherent Gore-Tex mesh is sewn to the fascial edges completely bridging the defect under moderate tension. Ideally the skin is closed over the Gore-Tex and drains are placed. The second stage is a series of multiple operative trips to serially excise the central piece of Gore-Tex (usually no more than 4 cm in width). This process gradually pulls the rectus muscles and the fascia back to the midline. In the final operation, the last piece of Gore-Tex is removed, a separation of parts is performed, the closure is usually reinforced with mesh underlay or overlay, and the skin is closed on top (see Figs.13-7, p. 237; 13-8, p. 239; and 13-12, p. 243)
2 Tissue Expansion
2 Choice of Tissue Expander Size, Shape, and Location
Fortunately today there are many options for tissue expansion. Multiple companies have premade expanders of all shapes and sizes and also have the ability to custom fabricate expanders of almost any desired dimensions. Most of the expanders come with remote ports, but several are also fitted with integrated ports. These ports are all composed of self-sealing silicone rubber backed by stainless steel and can be located by magnetic sensing devices placed over the skin. The length of the expander must match the length of the wound, and the height of the expander ideally should match the width (or when opposing symmetric expanders are placed, the height should match half the width). I prefer rectangular expanders for most defects except in the case of circular or elliptical defects where there is a large discrepancy in the width of the wound at the center versus either end. In those cases, a crescenteric expander is the ideal choice. Fill volume is not extremely important because the expanders are designed to tolerate overfilling by several times the official recommended volume. The placement location of the expander in the abdominal wall is not as complicated as it is in scalp expansion (for instance). In most instances, the expander or expanders will be adjacent to the long access of the defect. Care must be taken to visualize the final closure of the wound in order to properly place the expanders and subsequently close the defect with a minimum of disfiguring scars.
3 Operative Steps
1 Tissue Expansion and Closure of Abdominal Wall Skin
 Insertion of Tissue Expanders
Insertion of Tissue Expanders
After the abdominal wall has been analyzed and the expanders chosen and ordered, the first operation for insertion of the expanders is performed (Fig. 13-2, A-D and Fig. 13-3). The patient is asked to bathe with antimicrobial soap the night before the surgery (if practical). On the day of surgery, intravenous (IV) antibiotics are administered, and sequential compression devices are applied before induction. The wound should be prepped with alcohol and chlorhexidine because this provides the most effective antimicrobial barrier and the longest duration of action.

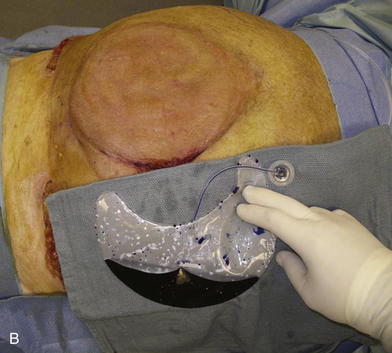

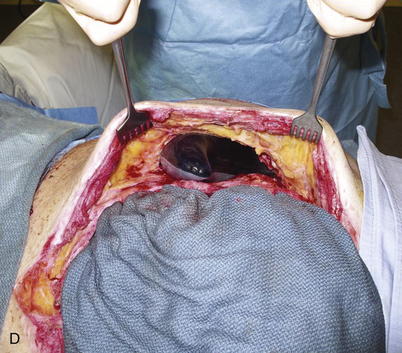
It is a natural instinct to place the incision for the expander at the edge of the wound to be closed. While this may work, it also subjects the incision to the forces of expansion and can lead to wound dehiscence and expander extrusion. I thus prefer to make a separate incision perpendicular and lateral to the long axis of the wound (see Fig. 13-2, A, and Fig. 13-3
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


