Chapter 6 Tip Sutures
 Video Content
Video Content Animations
AnimationsIn this Chapter Online at experconsult.com
Online Contents
Placing an Interdomal Suture Video 6.1
Use of an Interdomal Suture Animation 6.1
Placing a Transdomal Suture Video 6.2
Use of a Transdomal Suture Animation 6.2
Placing a Medial Crura Suture Video 6.3
Use of a Medial Crura Suture Animation 6.3
Repositioning of Basal Unit Anteriorly Animation 6.4
Placing a Tebbetts Lateral Crura Spanning Suture Video 6.4
Use of a Medial Crura–Septal Posterior Anchor Suture Animation 6.5
Use of a Tip Rotation Suture Animation 6.6
Use of a Lateral Crura Spanning Suture Animation 6.7
Use of a Lateral Crus Convexity Suture Animation 6.8
Pearls
• The tip sutures have a specific purpose to serve. However, there are often some unintended changes that occur, an understanding of which is crucial to provide a successful outcome.
• To change the shape of the cartilage, an absorbable suture material lasting only a few weeks, as opposed to a permanent suture, is sufficient.
• Whenever the suture has to overcome a continuous force such as gravity, for instance in tip rotation, permanent suture material is more reliable.
• The interdomal suture will narrow the tip, strengthen the tip support, increase the lobule volume, reduce the overall tip width and eliminate any clefting that may exist between the domes.
• The transdomal suture, besides narrowing the tip, will result in increase in tip projection, gain in infratip volume, flattening or concavity of the lateral crus, and reduction in interdomal distance.
• If the transdomal suture is placed caudally, it will rotate the lateral crus caudally; if it is placed cephalically, it will rotate the lateral crus cephalically.
• The middle and medial crura suture can be placed caudally, cephalically, or in the mid-portion of the width of the medial crura.
• The middle and medial crura suture narrows the width of the columella, reduces the interdomal distance, creates more stability in the central portion of the basilar nasal tripod, rotates the lateral crura caudally if it is placed along the caudal border of the medial crura or cephalically if it is placed along the cephalic border of the middle crura.
• The medial crura suture widens the nostrils and may cause some fullness caudally.
• The anterior medial crura-septal anchor suture will increase the tip projection, separate the domes slightly if they are not sutured to each other, rotate the tip cephalically, widen the nasolabial angle and elongate the columella and nostrils.
• The posterior medial crura-septal anchor suture not only reduces the tip projection, it will also result in narrowing the distance between the domes if they have not been stabilized, and will rotate the tip caudally, and shorten the columella and the nostrils.
• The tip rotation suture not only rotates the tip cephalically, it may retract the columella minimally.
• The lateral crura spanning suture is used to reduce the convexity of the lower lateral cartilages. It also narrows the distance between the domes, retracts the ala, and elongates the central portion of the nose.
• The lateral crura convexity suture alters convexity, resulting in slight elongation of the nose and a better tip.
• The footplate suture is used to reduce the distance between the divergent plates, which also creates more stability in the central portion of the nasal base tripod and advances the subnasale caudally; it reduces the effectiveness of the depressor nasi septi muscle.
• Complications of suture technique include too much narrowing of the tip, alar retraction, infection, palpability and extrusion.
Joseph first described the use of a suture technique to lessen the distance between the domes and also to rotate the tip cephalically by anchoring the medial crura to the caudal septum. He called this the ‘orthopedic suture’ and first published his work in 1931.1 Multiple sutures have since been described addressing specific problems related to the nasal tip and septal curvature. Some of the earlier tip sutures were used to correct cleft lip nose deformity by repositioning the distorted lower lateral cartilages and domes.2 McCullough3 and Tardy4 described the initial forms of the transdomal suture, which is used very commonly today to control the width of the domal arches. Daniel5 and Tebbetts6,7 additionally refined tip sutures. Gruber described the lateral crura convexity suture in 19978,9 and the author10 described the sutures that control the footplates. In a comprehensive review, the author discussed the goal of each suture and outlined the variety of changes that occur as a result of each suture, which may or may not be part of the aesthetic goals.11,12
Essentially every tip suture can be placed through an endonasal approach. However, an open approach provides a better opportunity to place the sutures more precisely and with greater ease. In this chapter, we will describe each suture and its intended objective and the different dynamic changes that each suture may induce. It is crucial to understand that these sutures cannot be used interchangeably and that each suture has a well-defined function and is designed to achieve a precise objective. It is also of paramount importance to recognize the multiple interplays resulting from each suture, which can be synergistic, antagonistic or unrelated to the overall aesthetic goals of rhinoplasty. Up to 3 years ago in the author’s own practice, in the absence of evidence-based knowledge regarding the lasting effects of sutures, many suturing techniques were carried out using permanent suture material. However, a study conducted by the author’s research team demonstrated that sutures that last six weeks or more can provide as enduring a result as those that are permanent.13 Armed with this information, the author’s current practice is to use 5.0 PDS for reshaping the tip cartilages, except for the tip rotation and suspension suture, where the goal is to eliminate the distance between the medial crura and the anterocaudal septum as well as to overcome the continuous force of gravity and the depressor septi nasi muscle on the tip in a lasting manner. For this, 5-0 clear nylon is used.
Tip Sutures
Interdomal Suture
Technique
A 5-0 PDS suture is placed in such a manner that the knot will end up underneath the domes. This suture can be placed as a simple loop or in a figure-of-eight fashion. A loop stitch (Figure 6.1, Animation 6.1, Video 6.1) may overlap the domal cartilages, while the figure-of-eight suture will not only avoid this but, if the domes are overlapping or are misaligned cephalocaudally, will align them.
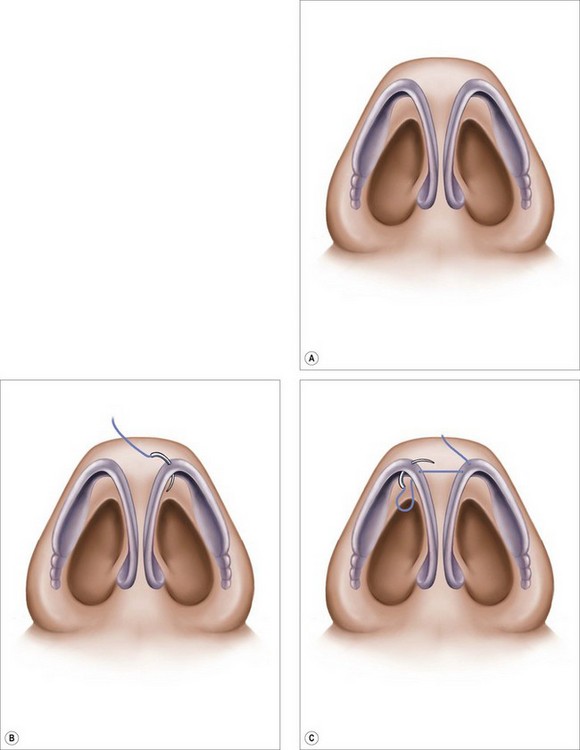
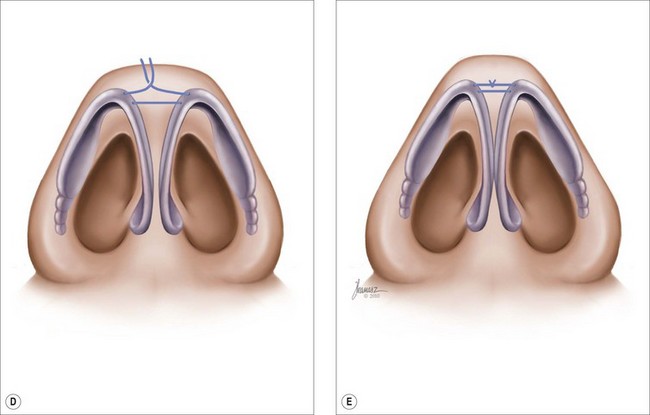
Figure 6.1 A 5-0 PDS suture is placed in such a manner that the knot will end up underneath the dome. 
 Animation 6.1 •
Animation 6.1 • Video 6.1 •
Video 6.1 •






