(1)
Department of Neurosurgery Faculty of Medicine, Saga University, Saga, Japan
Keywords
Retrosigmoid lateral suboccipital approachVariations of the approachInfratentorial lateral supracerebellar approachInfrafloccular approachTranscondylar fossa approach9.1 Introduction
Several approaches to lesions in the cerebellopontine angle (CPA) have been employed [3, 10, 11, 14, 19, 21, 22, 25]. Of these, the retrosigmoid lateral suboccipital approach (LSA) is the most convenient and frequently used. Because the bony opening is simple and intraoperative orientation easy, this approach is familiar to many neurosurgeons. LSA encompasses several approaches that vary in the application and positioning of bony openings depending on lesion location and the nature of each case. Figure 9.1 demonstrates two intraoperative views through LSA: first, a case of petrous apex meningioma in the upper CPA and second, a case of jugular foramen neurinoma in the lower CPA. Figure 9.1a, b shows the different operative views of the left CPA using the same approach.
Fig. 9.1
Illustrations showing different operative views through the LSA (from Matsushima T [10] with permission). (a) A meningioma around the Meckel’s cave viewed through the infratentorial lateral supracerebellar approach. (b) A jugular foramen neurinoma viewed through LSA
In this chapter, we briefly explain the basic procedure of the conventional LSA. Next, we describe in detail four variations of this approach based on the region of the CPA exposed, positioning of the bony opening, techniques employed, and positioning of the patient [3, 20, 21]. We also discuss special anatomical factors that make surgeries in CPA difficult and the limitations of surgeries in this region and comment on methods and techniques to resolve these difficulties. With regard to the basic anatomy of CPA, refer to Chap. 8: “The Cerebellopontine Angle: Basic Structures and the ‘Rules of Three.’”
9.2 Anatomical Limitations in Cerebellopontine Angle Surgeries
The following factors make surgeries in CPA difficult:
The posterior fossa is compact, and the working space is extremely narrow, particularly in cases of huge mass brain tumor and increased intracranial pressure.
Using LSA, lesions can be observed only after the cerebellar hemisphere is precisely retracted. However, cerebellar retraction occasionally causes swelling of the cerebellar hemispheres.
Numerous cranial nerves (CNs) and superior petrosal veins (Sup. Pet. Vs.) are obstacles, impeding both retraction of the cerebellar hemispheres and the access to regions deep to these nerves and veins. CN damage readily causes neurological deficits, such as hearing disturbances or difficulty swallowing, whereas Sup. Pet. V. damage rarely causes serious venous-related complications [8, 23].
Because the medial wall of CPA is the brainstem, which is critical to life, care should be taken to prevent surgical complications that may easily cause serious postoperative neurological deficits.
9.3 Basic Procedure of the Conventional Lateral Suboccipital Approach
9.3.1 Positioning, Head Posture, and Lumbar Drainage of Cerebrospinal Fluid
Although positions such as the lateral, prone, or sitting positions can be used, we prefer the lateral recumbent position because the sitting position carries the risk of air embolism. However, in the lateral recumbent position, the patient’s shoulder on the side of the lesion obstructs the surgeon’s hand and the other shoulder impedes the tilting of the patient’s head (Fig. 9.2a). Therefore, the upper limb that is opposite side of the lesion should not be supported by the operating table (Fig. 9.2b). To minimize this inconvenience, it is preferable to tilt the patient slightly forward, as in the prone position, instead of maintaining a complete lateral position (Fig. 9.2c, d). The term lateral position encompasses several positions with slight variations in body and head postures, depending on the surgical approach. For example, the lateral position in the infratentorial lateral supracerebellar approach for trigeminal neuralgia (TN) is different from that in the infrafloccular LSA for hemifacial spasm (HFS). In the latter approach, the body is rotated slightly anteriorly and the neck is tilted to the side opposite the lesion as much as possible to avoid obstruction by the patient’s shoulder and to facilitate observation from the posteroinferior side [17]. When it is necessary to make a horseshoe-shaped skin flap, the patient’s body and head are rotated more anteriorly, almost similar to the prone position [11].
Fig. 9.2
The lateral recumbent position. (a) Illustration showing a patient in the lateral position, with his or her upper limb supported by the operating table. (b) Illustration showing a patient in the lateral position, with his upper limb unsupported by the operating table. Without this support, the patient’s head can be tilted more inferiorly. (c, d) Photographs showing a patient in the lateral recumbent position in the operating room. The head and upper body are tilted slightly anteriorly to prevent obstruction of the surgeon’s hand by the patient’s left shoulder
Exclusion of cerebrospinal fluid (CSF) is crucial in LSA. Adequate exclusion of CSF relieves the tension on the cerebellum, thus reducing postoperative cerebellar hemorrhage. Among the methods of CSF exclusion, we regularly employ lumbar drainage before surgery. CSF exclusion through lumbar drainage is reliable and useful because the cerebellum is already relaxed when the dura mater is opened and the cerebellar hemisphere is retracted. CSF can also be aspirated from the cerebellomedullary cistern during surgery.
9.3.2 Skin Incision and Bony Opening
We usually make a linear skin incision, positioned several millimeters medial to the hairline behind the external auricle, facilitating easy exposure of the posterior margin of the sigmoid sinus. The inferior portion of the incision should be curved medially to avoid obstruction of the operative microscope by the medial side of the muscle flap [17] (Fig. 9.2b). In the transcondylar fossa or transcondylar approach, the prone position may be employed because a horseshoe-shaped skin incision is easy and safe [11, 25].
A bony opening is made along the posterior margin of the sigmoid sinus and the inferior margin of the transverse sinus, from the height of the transverse sinus to that of the jugular foramen. The margins of the sinuses should be exposed to reduce retraction of the cerebellum. The size of the bone window varies in each case. For example, a large bone window is preferable for a large acoustic tumor; half the ipsilateral cerebellar hemisphere is exposed and injury of the cerebellar hemisphere by the retraction is avoided. A large bone window makes surgery easy and safe and enables accurate orientation. Variations in bony opening and site will be explained in detail along with the variations of LSA.
9.3.3 Exposure of the Entire Cerebellopontine Angle
CSF should first be aspirated from the cerebellomedullary cistern. The arachnoid membrane is first incised near the jugular foramen below the flocculus because of the absence of Sup. Pet. Vs. in this region. While the membrane is incised, care should be taken not to injure Sup. Pet. Vs., particularly in the region superior to the flocculus, until the fissures in CPA are almost exposed. In most cases, we begin the incision of the arachnoid membrane in front of the jugular foramen using the lower CNs as anatomical landmarks (Fig. 9.3a). Subsequently, we gradually move superiorly, locating Sup. Pet. Vs. around the superior limb of the cerebellopontine fissure or on the upper part of the petrosal (lateral) cerebellar surface (Fig. 9.3b, c). At this stage, CNs VII and VIII are partially visible. It is often beneficial to observe the tentorial (superior) cerebellar surface for anatomical orientation. The process of exposing the entire CPA involves the exposure of all tributaries of Sup. Pet. V. Figure 9.3 illustrates the complete process of exposing the entire CPA (Fig. 9.3).
Fig. 9.3
Procedure of the basic approach. (a) Exclusion of cerebrospinal fluid after dissecting the arachnoid membrane in the cerebellomedullary cistern. (b) Exposure of the cranial nerves in the left CPA. (c) Exposure of tributaries of the Sup. Pet. V. When the arachnoid membrane around Sup. Pet. V. is removed from the inferolateral side, all tributaries are gradually exposed. Finally, the tributaries from the four different areas become clearly visible. The vein of the cerebellopontine fissure is the largest and often becomes a common stem. (d) Exposure and utilization of two cerebellar surfaces: the petrosal and tentorial surfaces. The two cerebellar surfaces should be exposed to obtain good orientation. The tentorial surface is more often used in surgeries of the upper CPA around CN V though the infratentorial lateral supracerebellar approach
9.4 Four Variant Approaches Depending on Four Separated Small Spaces and the Nature of Lesions
CPA is divided on the basis of CNs into the following four small spaces (Fig. 9.4a–c):
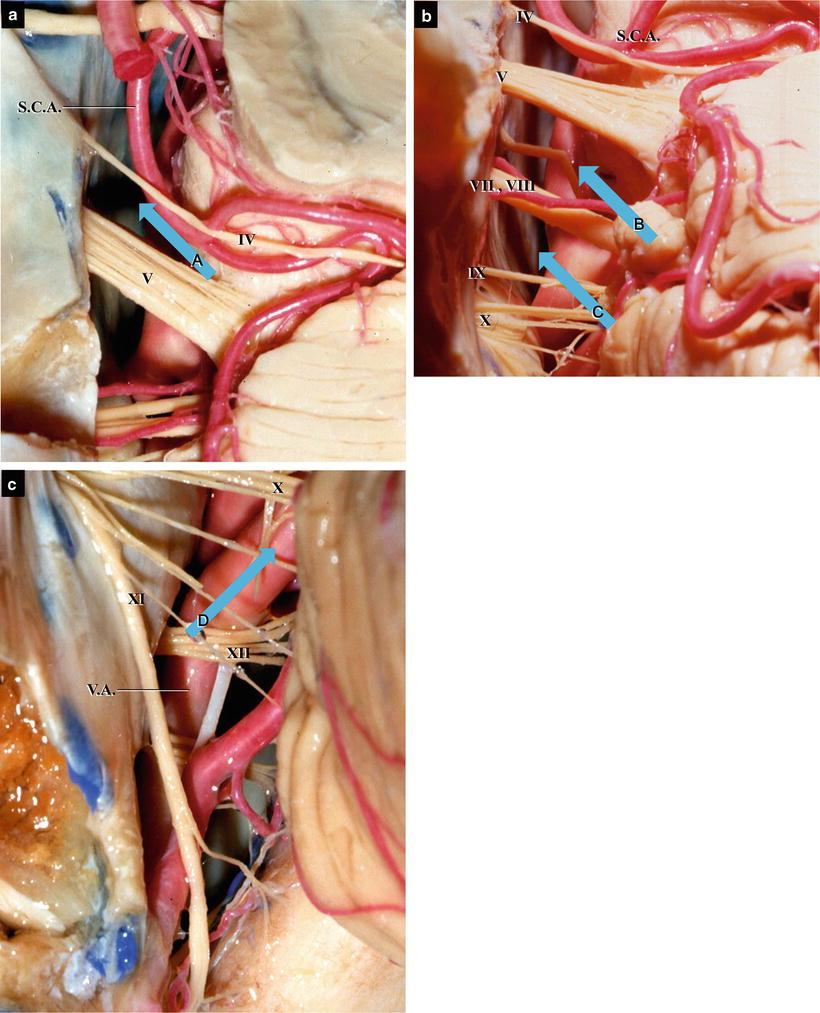
Fig. 9.4
Four areas of the cerebellopontine cistern divided on the basis of their relationship with the CNs (from Matsushima T et al. [18] with permission). A, the area superomedial to CN V; B, the area between CNs V and VII; C, the area between CNs VIII and IX; D, the area below CN X. (a) The upper portion of the CPA. (b) The middle portion of CPA. (c) The lower portion of CPA
A space medial to CN V
A space between CN V and CNs VII and VIII
A space between CNs VII, VIII, and IX
A space below the lower CNs
To reach lesions deep to the above CNs, it is necessary to traverse one of these four spaces. Considering the nature of the lesions and the four small spaces, the following variations of LSA are appropriately selected (Fig. 9.5) [3, 18, 21]:
Fig. 9.5
Diagrams of the four variations of the left LSA. (a) The infratentorial LSA (from Hitotsumatsu T et al. [3] with permission). (b) The infrafloccular LSA (from Hitotsumatsu T et al. [3] with permission). (c) The transcondylar fossa approach (from Hitotsumatsu T et al. [3] with permission). (d) Conventional LSA
The infratentorial lateral supracerebellar approach to the Meckel’s cave, often employed in microvascular decompression (MVD) for TN (Fig. 9.5a) [14, 15]
The infrafloccular LSA to CN VII in the supraolivary fossette, often employed in MVD for HFS (Fig. 9.5b) [3, 10, 17, 20, 21]
The transcondylar fossa or far lateral approach to the anterolateral medulla oblongata, often employed in MVD for glossopharyngeal neuralgia (GPN), direct surgeries of vertebral artery (VA) aneurysms, or removal of tumors in the cerebellomedullary and/or premedullary cisterns (Fig. 9.5c) [2, 4, 5, 9, 11, 16, 25–27]
The conventional LSA, used for large CPA tumors, such as large acoustic tumor or petrous apex meningioma, to allow exposure of the entire CPA (Fig. 9.5d)
The infratentorial LSA involves traversing the infratentorial subdural space on the lateral tentorial cerebellar surface medial to Sup. Pet. Vs. along the anterolateral margin to explore CN V, the Meckel’s cave, and the posterolateral surface of the midbrain. This approach is often used in cases of TN and tumors in the upper CPA. The approach has a few advantages: there are no obstacles and it avoids the CN VII and VIII complex and the vein of the cerebellopontine fissure, a major common stem of Sup. Pet. V. The infrafloccular LSA facilitates the observation of the supraolivary fosette, especially the exit zone of CN VII from the posteroinferior side through a space between the flocculus and CN IX. The choroid plexus protruding from the foramen of Luschka provides an anatomical landmark. The spatula tip is placed on the choroid plexus, and the inferior portion of the flocculus should be retracted superiorly because the proximal portions of CNs VII and VIII are hidden by the flocculus. The proximal portion of the anterior inferior cerebellar artery (AICA) and its relationship to the exit zone of CNs VII and VIII are clearly visible. In this approach, the arachnoid membrane, rhomboid lip, and/or choroid plexus around the lower CNs are first dissected and the lateral portion of the cerebellomedullary fissure (CMF) is appropriately opened, facilitating easy and safe retraction of the lower petrosal cerebellar surface. Without strong traction of the cerebellar hemisphere, the lower CNs and exit zone of CN VII can be observed and postoperative hearing disturbance can be avoided. This approach is used not only in MVD for HFS but also when attempting to locate the proximal portion of CN VII during acoustic tumor surgery.
The transcondylar fossa approach facilitates surgery through the spaces between the nerve fibers of CNs X–XI after extradural removal of the condylar fossa and posterior portion of the jugular tubercle. Because the intervals between the CN XI nerve fibers are wide enough to pass, this anatomical structure makes the surgery easy and safe. The approach has a few other advantages: the intracranial portion of VA is secured during the early stages of the surgery, allowing manipulation of microsurgical instruments along or parallel to VA, thus making the surgery easy and safe. Therefore, the approach is suitable for various surgeries, such as those for VA–posterior inferior cerebellar artery (PICA) aneurysms and MVD for GPN [9, 16, 25, 26]. Furthermore, tumors can be removed between the nerve fibers of CN XI and VA, minimizing postoperative complications associated with the lower CNs. The entire course of CNs IX and X in the cerebellomedullary cistern is easily observed, making this approach suitable in MVD for GPN [4, 16]. In addition, when opening of the ipsilateral CMF is combined with the approach, the cerebellomedullary cistern can be further exposed [6, 24].
The conventional LSA resembles a combination of the infratentorial lateral supracerebellar approach and the infrafloccular LSA. It offers a wide operative field, from CN V near the tentorial edge to the lower CNs in the cerebellomedullary cistern. It is therefore suitable for the removal of large tumors such as acoustic neurinomas or CPA meningiomas. The size of the bony window is decided after considering the bulging of the cerebellar hemisphere through the dural opening. Even through this approach, it is preferable to expose the transverse sinus widely, allowing the surgeons proceed a little farther from Sup. Pet. Vs. and the CN VII and VIII complex during the initial stages of the procedure and allowing the anterior side of the tumor to be observed through the infratentorial lateral supracerebellar approach [30].
9.5 Craniotomy: Differences in the Site and Size of Bone Windows in the Four Approaches
To efficiently employ the four approaches described above, the site, size, and shape of craniotomy should be selected on the basis of the approach (Fig. 9.6a) [3, 10, 20, 21
 The Veins of the Posterior Cranial Fossa: Nomenclature
The Veins of the Posterior Cranial Fossa: Nomenclature
 The Cerebellopontine Angle: Basic Structures and the “Rules of Three”
The Cerebellopontine Angle: Basic Structures and the “Rules of Three”
 Microvascular Decompression Surgery for Hemifacial Spasm: The Lateral Suboccipital Infrafloccular Approach
Microvascular Decompression Surgery for Hemifacial Spasm: The Lateral Suboccipital Infrafloccular Approach
 Occipital Artery–Posterior Inferior Cerebellar Artery Bypass Surgery
Occipital Artery–Posterior Inferior Cerebellar Artery Bypass Surgery
 Microvascular Decompression for Glossopharyngeal Neuralgia: Surgical Approaches Depending on the Offending Artery
Microvascular Decompression for Glossopharyngeal Neuralgia: Surgical Approaches Depending on the Offending Artery
 Microsurgical Anatomy of the Cerebellomedullary Fissure and Variations of the Transcerebellomedullary Fissure Approach
Microsurgical Anatomy of the Cerebellomedullary Fissure and Variations of the Transcerebellomedullary Fissure Approach




Related posts:
The Veins of the Posterior Cranial Fossa: Nomenclature
The Cerebellopontine Angle: Basic Structures and the “Rules of Three”
Microvascular Decompression Surgery for Hemifacial Spasm: The Lateral Suboccipital Infrafloccular Approach
Occipital Artery–Posterior Inferior Cerebellar Artery Bypass Surgery
Microvascular Decompression for Glossopharyngeal Neuralgia: Surgical Approaches Depending on the Offending Artery
Microsurgical Anatomy of the Cerebellomedullary Fissure and Variations of the Transcerebellomedullary Fissure Approach
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
