6 The Progressive Peel
The Combined Jessner, TCA, Retinoid Peel
Introduction
In our evolution of chemical peeling for all skin types we have developed the progressive peel. This is a multiple coat peel in four steps, allowing the operator to watch the skin and adjust the peel to the skin’s reaction. Some patients will require three or four coats of each progressive peel solution I, II, III and IV. Other patients will develop the end point of the rosy red hue with a white frost with several coats of progressive peel I or II. This gradual progression of the peel allows the operator to stop at a safe end point. The step-by-step process avoids alabaster white, yellow or grey frost that may occur with high concentrations of TCA (45–55%) applied in one or two coats. Historically, the suggestions of other progressive peelers still apply (Box 6.1).
Box 6.1
Suggestions from Eller and Wolff – (1941)
This chapter will be an overview of this progressive peel. We outline the step-by-step skin rejuvenation program (Box 6.2) for the improvement of complexion problems, fine lines and/or blotchy dyspigmentations in 155 patients. This illustrates what types of patients will benefit from the progressive peel. Afterwards, you will be able to conduct your patients through this step-by-step program to a freshened complexion. Previous authors in this textbook have also discussed skin preconditioning before the peel and more penetrating peels are covered in later chapters (see Box 6.3).
Box 6.3
Key features
Method
• Patient selection
Skin Analysis
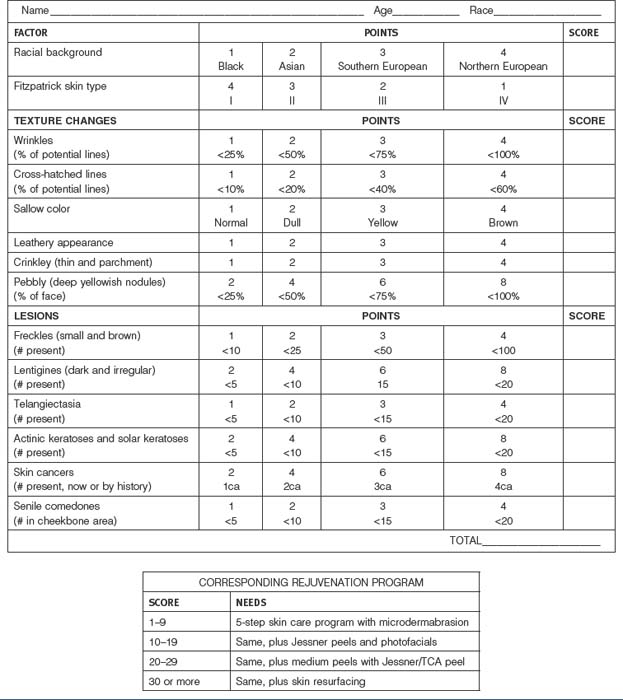
The skin analysis is the starting point for this rejuvenation process. The patient is classified by their Fitzpatrick skin type, plus, the extent of wrinkling, blotchy dyspigmention, sallow color, telangiectasia, pebbly appearance and the presence of skin lesions such as actinic keratoses. The overall score dictates the extent of skin rejuvenation required (Box 6.4). These findings correlate with the Rubin photo aging index. Rubin Level I is characterized by epidermal findings that maybe corrected with an aggressive topical skin care program alone. Rubin Level II is associated with papillary dermal findings which require a daily skin care program plus the progressive peel. Ruben Level III is with reticular dermal level changes which may require deeper rejuvenations such as laser resurfacing, dermabrasions or phenol peels. These will be covered in later chapters.
Informed Consent
The risks and benefits of this step-by-step skin rejuvenation program and the risks and benefits of alternative treatments including no treatment at all are discussed with the patient. All their questions are answered. These peels are contraindicated in some patients (Box 6.5). The degree of skin damage is determined and further documented with digital photography. Each patient signs the informed consent.
• The step-by-step skin rejuvenation program (Box 6.2)
Steps II and III will continue for 4 to 16 weeks depending upon the skin type (Box 6.6) For example, the skin conditioning must be longer in the darker skin types to reduce the possibility of dyschromias.
• The progressive peel
Tray Setup
A standard tray set up is important so nothing will be missed (Figure 6.1). Well-marked containers are used for the four peel solutions. Folded 3″ × 3″ cotton gauze is used to scrub in the chemical solutions. Five or six mL of each solution is poured onto the gauze which is rung out before the application begins sp the solution does not drip, cotton tipped applicators are available for small areas that require touch-ups or for around the eyes or temple areas. An eye wash solution is always on the tray to irrigate the eyes, if necessary. A bottle of water is on the tray to remind the patient to drink 4 or 5 glasses during the day to flush out any penetrating chemicals.









