CHAPTER 11 The Direct Anterior Approach



PREOPERATIVE PLANNING
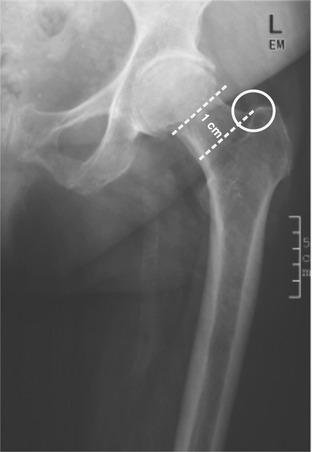
Templating of implant types and sizes should be performed as usual. The only difference between the direct anterior approach and other approaches is that with the direct anterior approach the osteotomy is performed without dislocating the hip joint. This is why this approach requires a precise definition of the starting point of the osteotomy. This point is found on the anteroposterior radiograph in the saddle that connects the femoral neck with the greater trochanter area and can be easily identified in situ (Fig. 11-1).
TECHNIQUE
Patient Positioning
The patient is placed in the supine position on the operating table. A table attachment opposite to the operated side (e.g., an armboard) will make hyperabduction of the opposite leg during femoral exposure easier. Both legs should be draped in a manner that allows flexibility in manipulation. This allows the surgeon to cross the operated leg under the opposite leg during the surgical exposure of the femur and facilitates the change to the opposite side if a bilateral total hip arthroplasty is performed (Fig. 11-2).




Portal
The anterior superior iliac spine and the greater trochanter are palpated (Figs. 11-3 and 11-4). The proximal starting point is found two fingerbreadths laterally and two fingerbreadths distally to the anterior superior iliac spine. The initial incision should be kept small (6-7 cm) and extended as needed.
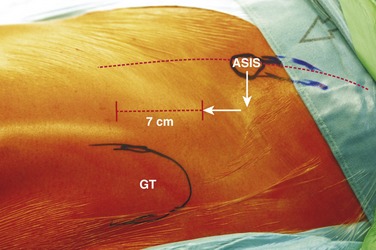
FIGURE 11-3 Coordinate system for the skin incision using the anterior superior iliac spine (ASIS) and the greater trochanter (GT) as starting points. The lateral femoral cutaneous nerve is in the area of this approach; placing the incision as laterally as possible protects that nerve. In the area of the incision, vessels perforating the iliotibial band can be found and must be cauterized (see Fig. 11-4).

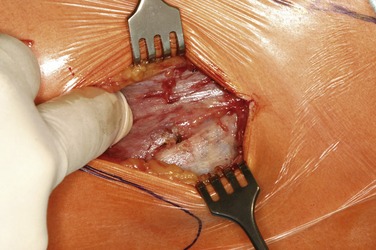
One must avoid cutting into the tensor fasciae latae before precisely locating the correct portal. The index finger can be used in proximal to distal movements to palpate the interval between the tensor fasciae latae and sartorius (Fig. 11-5). An alternative technique is to identify the fascia of the gluteus medius muscle; it has consistently a whiter, more fascial appearance. The muscle immediately medial to this is the tensor fascia.