CHAPTER 17 The Cemented Stem
KEY POINTS
 Cemented stems are indicated in patients who require a hip arthroplasty for all pathologic processes in all age groups.
Cemented stems are indicated in patients who require a hip arthroplasty for all pathologic processes in all age groups.



INDICATIONS AND CONTRAINDICATIONS
Cemented femoral stems can be considered for any patient who requires a hip arthroplasty. Force-closed or taper-slip designs have generally given better results than shape-closed implants.1 In complex cases in which there is distortion of the anatomy, femoral shortening procedures and derotation osteotomies can be carried out. The osteotomy sites should be cleared of cement or protected from cement intrusion by the use of impacted bone chips. Cemented hemiarthroplasties or cemented femoral components in total hip arthroplasties are indicated for displaced fractures of the femoral head. In cases of previous septic arthritis of the hip, cement can be loaded with an appropriate antibiotic to reduce the risk of recrudescence of infection.
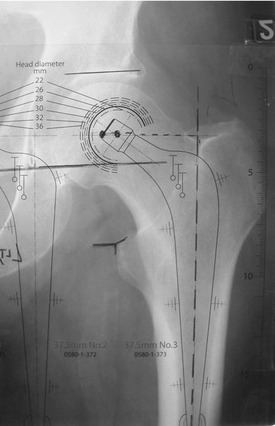
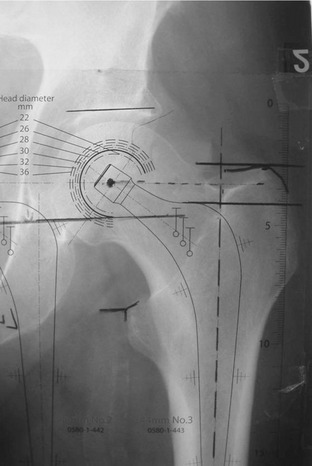
PREOPERATIVE PLANNING
For templating of conventional radiographs:
TECHNIQUE
The longevity of the femoral stem depends on establishing adequate initial mechanical interlock between the implant and the bone. A stable interface and osseointegration of the cement has been described in the long term.2 With cemented stems, a satisfactory interface is achieved by creating a “closed cavity” and then using contemporary cementing techniques to introduce and pressurize cement. By applying pressure on cement from initial injection up to the moment polymerization is complete, good cement intrusion into bone is ensured and blood is prevented from accumulating at the interface. A closed cavity is obtained by occluding the distal femoral canal with a plug. The strong cancellous bone that remains after broaching is thoroughly lavaged, and the canal is then filled in a retrograde fashion with the use of a cement gun. The proximal opening of the canal is sealed to allow the cement to be pressurized by continued use of the gun through the seal. Application of pressure is continued until the femoral component has been inserted and the cement has fully polymerized.
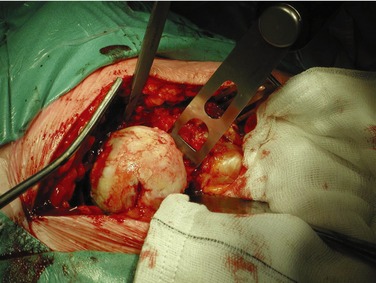
Femoral Neck Cut
The level of the neck cut is not critical with polished, double-tapered, collarless systems. The resection line usually runs from a point midway between the upper margin of the lesser trochanter and the inferior aspect of the femoral head to the upper surface of the base of the femoral neck where it meets the greater trochanter (Fig. 17-3).
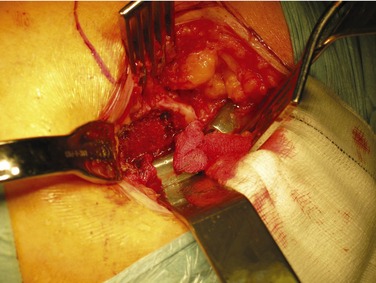
Femoral Exposure
The leg is internally rotated and the hip flexed to visualize the proximal femur. In routine cases neither the anterior capsule nor iliopsoas tendon requires release. Additionally, the piriformis muscle can often be preserved. A femoral elevator is placed on the anteromedial aspect of the neck to deliver the femur into the wound. A gluteus medius retractor is passed around the greater trochanter to retract the gluteus medius and minimus, and the other end of this retractor is held in place by a towel clip (Fig. 17-4). A weight and chain can be attached to any of these retractors to free the hands of the assistant. Exposure should be sufficient to allow a straight shot down the femur.