Innovative Technology for Knee Laxity Evaluation
Clinical Applicability and Reliability of Inertial Sensors for Quantitative Analysis of the Pivot-Shift Test
Keywords
• Knee kinematics • Anterior cruciate ligament injury • Dynamic instability • Pivot-shift test • Acceleration
Key Points
Introduction
Instability of the tibiofemoral joint secondary to an anterior cruciate ligament (ACL) injury is considered a critical issue and relates to the concept of joint laxity.1 By definition, laxity is the displacement, or the rotation, produced in response to an applied load or moment. Moreover, it is defined as static laxity when only one degree of freedom is involved and dynamic when more than two are considered.2
Because the ACL represents the primary restraint to tibia anteroposterior (AP) displacement,3 historically, the first approach to the evaluation of the tibiofemoral joint laxity involved the measurement of joint AP translation. From this point of view, Lachman and drawer tests are still the most commonly used tests to quantify the static laxity of the knee joint.
Although the previous tests are useful in the detection of a large part of ACL injuries, they do not provide information about rotational and dynamic laxity of the joint. Moreover, analyzing solely static laxity makes it difficult to isolate the injured ligament because of the different structures involved in the restraining phenomenon.4 Thus, additional stress tests have been introduced.
The pivot-shift (PS) phenomenon is commonly described as the anterior subluxation of the lateral tibial plateau followed by its sudden reduction during combined stresses.2,5 This pathway has been widely identified to be one of the essential signs of functional ACL insufficiency6,7; thus, clinicians have been trying to mimic it by means of a combination of valgus stress and tibial internal rotation during limb flexion.5,7
Lachman and PS are the two clinical tests most commonly used to assess knee laxity.8 Although the PS test could be considered the most specific test in detecting ACL injury,4,9,10 the Lachman test, involving only one knee grade of freedom, remains more easily quantifiable and sensitive.
Moreover, literature reported that PS grade more closely correlates with instability symptoms,11 reduced sport activity,12 articular cartilage damage, and meniscal damage13 with respect to the standard clinical examinations addressing only static joint laxity (ie, Lachman and drawer tests).14
The major problem using PS test lays in the complexity of the maneuver itself, which provokes a large variability both between testers and patients and making it a highly surgeon-subjective clinical examination.15–17 Furthermore, given that the test itself is a combined stress, PS test lacks a generally recognized quantitative and overall measurement.
Quantitative evaluation of the PS test
Thus, rather complex systems have been developed, using skin markers, force footplates, robotic technology, or image-based systems in dynamic condition, such as magnetic resonance imaging.18–21
Navigation Systems
Among the most commonly used systems, more recently, navigation systems have enabled surgeons to analyze the dynamic motion of the components associated with the PS phenomenon.4,10,22–28 Colombet and colleagues,29 Pearle and colleagues,30 and Lopomo and colleagues4 measured in in vivo and in vitro setups, respectively, the kinematic tests using a commercial navigation system, with an accuracy of within 1° and 1 mm. Lane and colleagues27 reported on correlations between clinical grading of PS and navigation data, defining the “p-angle,” described by the movement of the pathologic limb during PS test compared with a reference movement, finding a good correlation between this parameter and the clinical grade of the PS. As recently reported by Bignozzi and colleagues,10 the use of Computer Aided Surgery (CAS) system has been increased parallel to the development of double-bundle ACL reconstructions. Specifically, Lopomo and colleagues4 and Bignozzi and colleagues31 reported the use of navigation system in assessing dynamic laxity during anatomic double-bundle reconstruction, analyzing the kinematic behavior of the limb during the maneuver before and after surgery, and thus identifying specific parameters enabling the assessment of PS grade.
Despite the fact that the PS analysis obtained using navigation system provides a reliable and quantitative description of the test correlated with the clinical laxity classification,4 its application, because of the invasiveness, is however limited to the surgical site, preventing a side-to-side comparison. The only exception is the work of Miura and colleagues,32 in which knee-laxity between ACL-reconstructed knees and controlateral stable knees was compared intraoperatively by the use of a navigation system.
Toward Noninvasive Methodologies
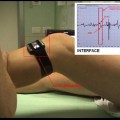
Several studies reported the use of electromagnetic sensors15,33–36 to quantitatively analyze the PS test. Bull and colleagues2 were the first to use electromagnetic systems with skin-mounted sensors. Similarly, Kubo and colleagues37 developed a noninvasive measurement system using commercial electromagnetic tracking system, finding a good correlation with bone-fixed measurements and identifying the velocity as a good parameter to grade PS test. Analogously, Hoshino and colleagues16,33,36
Related posts:
 Knee Laxity
Knee Laxity
 and Return to Play After Anatomic Anterior Cruciate Ligament Reconstruction
and Return to Play After Anatomic Anterior Cruciate Ligament Reconstruction
 Cruciate Ligament Healing and Advances in Imaging
Cruciate Ligament Healing and Advances in Imaging
 of Anterior Cruciate Ligament Reconstruction
of Anterior Cruciate Ligament Reconstruction
 in Surgeon Preferences on Anterior Cruciate Ligament Reconstructive Techniques
in Surgeon Preferences on Anterior Cruciate Ligament Reconstructive Techniques
 Technique for Anterior Cruciate Ligament Injury
Technique for Anterior Cruciate Ligament Injury
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


