Augmentation Technique for Anterior Cruciate Ligament Injury
Keywords
• Anterior cruciate ligament (ACL) • Augmentation technique • Partial rupture • Remnant-preserving technique • Double bundle
Key Points
Anterior cruciate ligament (ACL) reconstruction has become a common treatment in orthopedic sports medicine. The normal ACL consists of 2 major functional bundles: the anteromedial (AM) bundle and the posterolateral (PL) bundle. Traditional single-bundle ACL reconstruction has concentrated mainly on the functional restoration of the AM bundle.
Recently, several studies have shown that the central anatomic single-bundle ACL reconstruction can restore normal knee function.1–3 With this method, the tibial and femoral tunnels are well placed in the center of their respective ACL footprints. Moreover, interest in double-bundle ACL reconstruction has been growing because of its greater potential to restore knee kinematics.4–8 Double-bundle ACL reconstruction can mimic more closely the normal structure of the ACL. Restoration of the biomechanical function is essential in ACL reconstruction. However, biological healing of the graft is vital to the achievement of satisfying clinical results. Accelerated biological healing is necessary not only for early return to sports but also for reliable remodeling of the grafted tendon.
ACL augmentation
Potential Advantages
Arthroscopic examination for ACL reconstruction occasionally demonstrates a relatively thick and abundant ACL remnant. In standard single-bundle or double-bundle ACL reconstruction, the ACL remnant is totally debrided to enable clear visualization of the femoral and tibial bone tunnels. However, recent studies have shown that human ACL remnants contain several types of mechanoreceptors. These mechanoreceptors may provide positive effects on the proprioceptive function of the knee.9–12 In addition, some studies have shown that the ACL remnants provide some biomechanical stability to the knee.13,14 Therefore, ACL reconstruction that preserves the remnant by using the ACL augmentation technique might have several advantages:
Indications
The ACL remnant often maintains a bridge between the tibia and either the intercondylar notch or posterior cruciate ligament (PCL). Even when the substantial remnant maintains a bridge between the tibia and the intercondylar notch, the femoral attachment of the ACL remnant is often positioned abnormally. These cases represent a complete rupture of the ACL. However, sometimes a partial rupture of the AM or PL bundle of the ACL can be observed. In the authors’ previous studies, the frequency of partial rupture was 10% during 2002 and 2005,15 and 20% during 2006 and 2008.13 In these cases, although rupture of the AM bundle or PL bundle could be seen, the other bundle was well preserved, with an attachment of anatomic femoral origin.
Preoperative and Intraoperative Evaluation
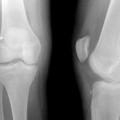
It is sometimes difficult to decide whether the remaining bundle represents a partial or complete rupture of the ACL. The decision was made after thorough consideration of physical, magnetic resonance imaging (MRI), and arthroscopic findings.13 Quantitative evaluation of anteroposterior knee laxity can be one indicator for this decision. Partial rupture of the ACL was suspected when the side-to-side difference in the anterior displacement of the tibia was less than about 5 mm and a delayed firm end point was noted. The anterior displacement of the tibia was measured by the KT-2000 knee arthrometer or Kneelax-3 at 30 lb (13.6 kg). MRI also provides important information for evaluation of the femoral attachment of the bundles. However, the final decision was made after arthroscopic confirmation of the status of the injured ACL.
Evaluation by Arthroscopy
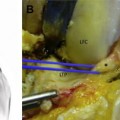
Arthroscopic intra-articular inspection was performed through the standard AM portal, anterolateral portal, and the far AM portal. A thorough arthroscopic probing is needed to precisely assess the ACL remnant patterns. Careful probing on the femoral side is important because most ACL ruptures occur in the proximal half. Partial rupture of the ACL was suspected when ligamentous continuous fibers were observed between the tibia and the anatomic femoral insertion of the ACL. Furthermore, arthroscopic examination should be performed in a figure-of-4 position and at various knee-flexion angles to consider the different tension patterns of the 2 bundles.16–19
Classification of the ACL Remnant
The ACL remnant pattern was thoroughly examined to determine the treatment strategy, and was classified (Box 1). Groups 1a and 1b indicate single-bundle reconstruction with the remnant-preserving technique. Groups 1c, 2a, 2b, and 2c indicate double-bundle reconstruction with the remnant-preserving technique. It is important for surgeons to keep in mind that, even in the partial rupture cases, the remaining bundle is invariably not completely intact. It is likely that the biomechanical function of the remaining bundle declines to some extent.
Box 1 Classification of the ACL remnant
Group 1: Partial rupture of the ACL
Group 2: Complete rupture of the ACL
Surgical technique
Since 1992, the senior author has performed the ACL augmentation technique when indicated.20 However, the early procedures required 2 incisions at the medial aspect of the proximal tibia and at the lateral femoral condyle, because the grafted tendon was fixed to the femur through the over-the-top route. This early technique had a serious flaw, because it was not a true reconstruction that restored normal ACL anatomy. Therefore, Ochi started to perform the 1-incision technique for ACL augmentation in 1996. Compared with the 2-incision technique, the 1-incision technique is less invasive and enabled reconstruction of the ACL in the anatomic portion. Here the authors introduce the ACL augmentation technique for partial and complete rupture of the ACL.15,21–23
Graft Preparation
Related posts:
 Knee Laxity
Knee Laxity
 and Return to Play After Anatomic Anterior Cruciate Ligament Reconstruction
and Return to Play After Anatomic Anterior Cruciate Ligament Reconstruction
 Cruciate Ligament Healing and Advances in Imaging
Cruciate Ligament Healing and Advances in Imaging
 Reconstruction and Extra-articular Tenodesis
Reconstruction and Extra-articular Tenodesis
 of Anterior Cruciate Ligament Reconstruction
of Anterior Cruciate Ligament Reconstruction
 in Surgeon Preferences on Anterior Cruciate Ligament Reconstructive Techniques
in Surgeon Preferences on Anterior Cruciate Ligament Reconstructive Techniques
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


