Chapter 19 Synthetic Mesh Choices for Surgical Repair
1 Introduction to Synthetic Mesh Materials
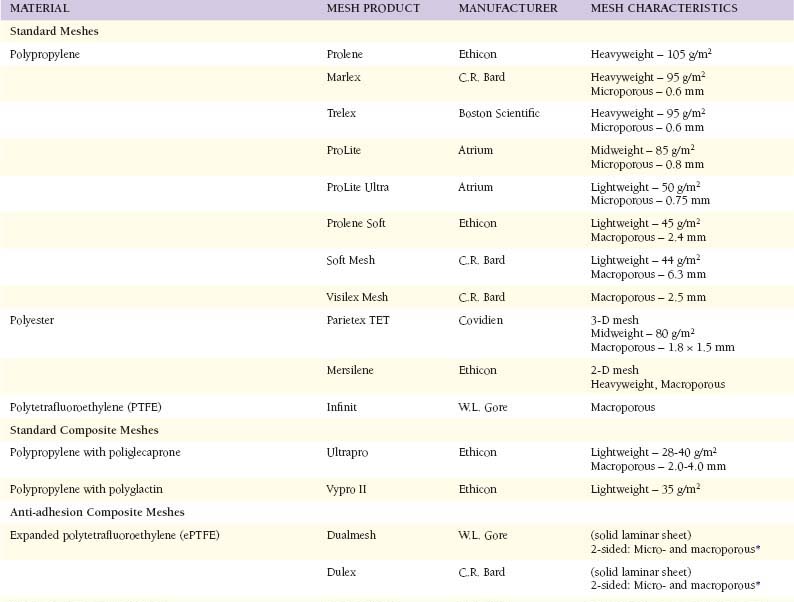
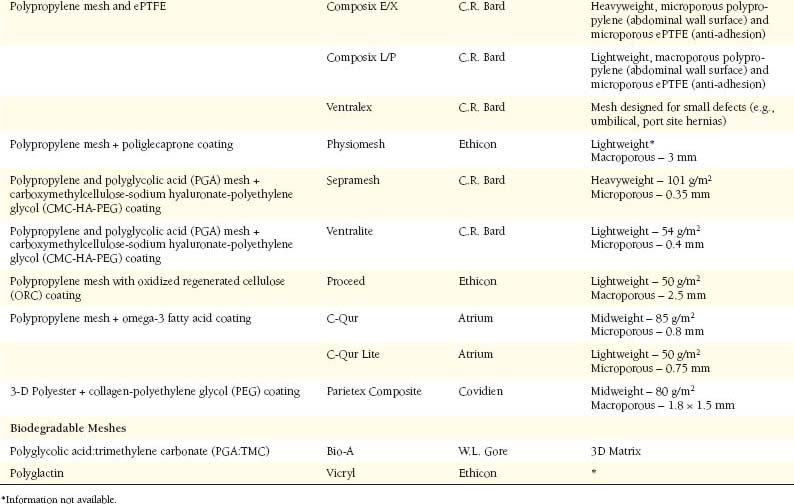
 Modern herniorrhaphy relies on the use of prosthetic implants to allow for tension-free repairs of hernia defects. Such widespread use of mesh implants has greatly reduced the incidence of hernia recurrence. Surgeons continuously seek the ideal mesh—pliable and durable with chemical inertness and limited immunogenicity. Synthetic meshes have been used for over half a century, since Dr. Francis Usher popularized the use of polypropylene in the late 1950s. However, only recently have there been any changes in their original design. Current manufacturing techniques involve modifications of mesh polymers, reduction in fiber density, increase in pore size, and combinations of the above in attempts to create an “ideal mesh” to replace native fascia during hernia repair.
Modern herniorrhaphy relies on the use of prosthetic implants to allow for tension-free repairs of hernia defects. Such widespread use of mesh implants has greatly reduced the incidence of hernia recurrence. Surgeons continuously seek the ideal mesh—pliable and durable with chemical inertness and limited immunogenicity. Synthetic meshes have been used for over half a century, since Dr. Francis Usher popularized the use of polypropylene in the late 1950s. However, only recently have there been any changes in their original design. Current manufacturing techniques involve modifications of mesh polymers, reduction in fiber density, increase in pore size, and combinations of the above in attempts to create an “ideal mesh” to replace native fascia during hernia repair.2 Mesh Characteristics (Table 19-1)
1 Material
 Polypropylene constitutes the most common polymer used in surgical meshes. It is highly durable and has been proved successful in hernia repairs for over 50 years. Because of unraveling at the edges when cut, current meshes are typically knitted instead of woven. While still popular because of its strength, durability, and pliability, polypropylene meshes are not without their drawbacks. Traditional polypropylene induces a strong inflammatory reaction upon implantation. Such inflammation can lead to excessive fibrosis, loss of pliability, and chronic pain. Additionally, when exposed to bowel, uncoated polypropylene may lead to extensive adhesions and/or fistulas.
Polypropylene constitutes the most common polymer used in surgical meshes. It is highly durable and has been proved successful in hernia repairs for over 50 years. Because of unraveling at the edges when cut, current meshes are typically knitted instead of woven. While still popular because of its strength, durability, and pliability, polypropylene meshes are not without their drawbacks. Traditional polypropylene induces a strong inflammatory reaction upon implantation. Such inflammation can lead to excessive fibrosis, loss of pliability, and chronic pain. Additionally, when exposed to bowel, uncoated polypropylene may lead to extensive adhesions and/or fistulas. Polyester is a hydrophilic polymer incorporated into meshes. It has been manufactured as a 2-dimensional (flat) sheet or a 3-dimensional sheet to allow for greater incorporation of host tissues. One of the advantages of polyester is its pliability, which allows the surgeon to easily manipulate and fixate the mesh to the conformations of the abdominopelvic walls. Polyester is unique in its hydrophilic nature; however, the clinical relevance of this feature remains unknown. Like polypropylene, unprotected polyester can lead to significant inflammatory reactions with ensuing fibrosis, adhesions, and fistulas.
Polyester is a hydrophilic polymer incorporated into meshes. It has been manufactured as a 2-dimensional (flat) sheet or a 3-dimensional sheet to allow for greater incorporation of host tissues. One of the advantages of polyester is its pliability, which allows the surgeon to easily manipulate and fixate the mesh to the conformations of the abdominopelvic walls. Polyester is unique in its hydrophilic nature; however, the clinical relevance of this feature remains unknown. Like polypropylene, unprotected polyester can lead to significant inflammatory reactions with ensuing fibrosis, adhesions, and fistulas.

2 Weight and Density
 Studies have shown that traditional “heavyweight” meshes demonstrate four times the tensile and burst strength of the native abdominal wall. As a result, traditional meshes may be overengineered for use in most hernia repairs. The latest generation of meshes has been designed to reduce the amount of implanted prosthetic material. These so-called lightweight meshes are manufactured with thinner filaments and/or larger pore sizes resulting in markedly reduced mesh “weights,” measured in grams per m2. Such reduction (>50%) in prosthetic weight potentially allows for a reduced inflammatory reaction, more flexibility, and improved compliance, especially in the long-term.
Studies have shown that traditional “heavyweight” meshes demonstrate four times the tensile and burst strength of the native abdominal wall. As a result, traditional meshes may be overengineered for use in most hernia repairs. The latest generation of meshes has been designed to reduce the amount of implanted prosthetic material. These so-called lightweight meshes are manufactured with thinner filaments and/or larger pore sizes resulting in markedly reduced mesh “weights,” measured in grams per m2. Such reduction (>50%) in prosthetic weight potentially allows for a reduced inflammatory reaction, more flexibility, and improved compliance, especially in the long-term.3 Porosity
 In addition to reducing fiber caliber and density, increasing the distance between the mesh fibers also contributes to overall foreign body reduction. Following implantation, each mesh fiber is surrounded by some degree of inflammation and fibrosis. Microporous mesh induces significant perifilamentous fibrosis that tends to blend together, creating a scar plate. As pore size is increased between fibers, less bridging fibrosis may be observed, with subsequent reduced scar plate formation. This results in improved fluid transport across the mesh, theoretically lessening seroma formation. Marlex is considered a microporous mesh, with a pore size of 0.6 mm. Ultrapro, one of the most macroporous meshes, contains pore sizes ranging from 2 to 4 mm (diagonal-shaped pores).
In addition to reducing fiber caliber and density, increasing the distance between the mesh fibers also contributes to overall foreign body reduction. Following implantation, each mesh fiber is surrounded by some degree of inflammation and fibrosis. Microporous mesh induces significant perifilamentous fibrosis that tends to blend together, creating a scar plate. As pore size is increased between fibers, less bridging fibrosis may be observed, with subsequent reduced scar plate formation. This results in improved fluid transport across the mesh, theoretically lessening seroma formation. Marlex is considered a microporous mesh, with a pore size of 0.6 mm. Ultrapro, one of the most macroporous meshes, contains pore sizes ranging from 2 to 4 mm (diagonal-shaped pores).




