CHAPTER 36 Surgical Approach to the Hip
Direct Lateral
KEY POINTS
 The direct lateral approach is an anterolateral approach to the hip that involves dissection through the gluteus medius and minimus.
The direct lateral approach is an anterolateral approach to the hip that involves dissection through the gluteus medius and minimus.



The direct lateral approach to the hip has been widely used for both primary and revision total hip arthroplasty. By definition the direct lateral approach to the hip involves entrance to the hip joint via a split in the gluteus medius and minimus. Many variations of the direct lateral approach have been described and are generally characterized by the amount of abductor mechanism released from the greater trochanter and whether the abductor is released directly or with a bony fragment. Perhaps the most widely popularized description of the direct lateral approach is the Hardinge variation.1 This approach was popularized with the introduction of the Porous Coated Anatomic (PCA) total hip arthroplasty system (Howmedica, Rutherford, NJ). The key feature of the Hardinge approach involves detachment of approximately 50% to 60% of the abductor mechanism from the greater trochanter. This feature facilitates exposure of both the acetabulum and the proximal femur for implant placement. For surgeons concerned about tendon-to-tendon healing, Dall described a technique of releasing the abductor with a bony fragment.2 At the conclusion of the operative intervention, the fragment was approximated with either suture or cerclage wire. The advantages touted for this variation were direct bone to bone healing. Since 1985 the current authors have used their own specific modification of the direct lateral approach. This modification was originally described in collaboration with our practice by Frndak and colleagues for primary total hip arthroplasty3 and by Head and colleagues for revision total hip arthroplasty.4 The essential difference in this modified technique involves the preservation of at least 60% to 75% of the attachment of the abductor mechanism to the greater trochanter. We release only 25% to 30% of the abductor from the greater trochanter. Therefore the major advantage of our modification is maintenance of a significant attachment of the abductor mechanism, which allows for a more rapid return of function and minimizes postoperative limping, one of the major criticisms of this technique.
INDICATIONS AND CONTRAINDICATIONS
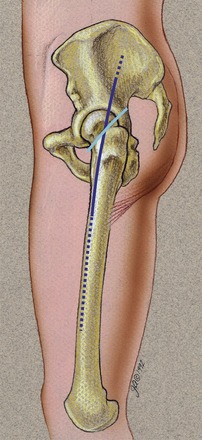
The direct lateral approach to the hip can be used for both primary and revision total hip arthroplasty (Fig. 36-1). It represents our preferred method of surgical approach. The major advantage of the direct lateral approach is the ability to effectively visualize both the acetabulum and the proximal femur. We have used this approach to perform simple primary total hip arthroplasty and have extended it to perform complex acetabular reconstruction and femoral reconstruction. The major advantage of the direct lateral approach as reported in nearly all literature on this topic is the postoperative stability afforded by the approach. This advantage has been clearly demonstrated in revision total hip arthroplasty. One of the more frequently performed current revision hip arthroplasties involves isolated acetabular liner exchange. Although liner exchange may appear to both the surgeon and the patient to be a relatively simple operative intervention, it has been plagued by postoperative dislocation when performed via a posterior approach. On the other hand, we have experienced a relatively low incidence of dislocation for isolated liner exchange when performed via a direct lateral approach.5 Our findings have been validated by several other reports. Therefore a specific indication for revision hip arthroplasty through a direct lateral approach would be isolated acetabular liner exchange in an effort to prevent the unwanted complication of dislocation. We use the direct lateral approach for all revision hip arthroplasties, even those that have been previously performed via a posterior approach. The only relative contraindication to our use of the direct lateral approach involves those cases in which total absence of any posterior soft-tissue structures of the proximal femur is noted on exposure. This posterior so-called “bald eagle” is more appropriately approached posteriorly with an attempt at soft-tissue reconstruction at the conclusion of the operative intervention.